 Neurological emergencies in Pediatrics
Neurological emergencies in Pediatrics  |
| Topics on Continuous Training |
H. Gómez Martín, M. Justel Rodríguez, A. Hernández Fabián
Pediatric Neurology Unit. University Hospital of Salamanca
| Abstract
Neurological emergencies are not the most frequent reason for attending Primary Care or Pediatric Emergency Departments. On many occasions, especially during our training, they can be difficult to deal with, generating some rejection and making us feel insecure in their management. Systematic assessment of these patients significantly helps their diagnosis and subsequent management. In most cases, a complete and detailed history and physical examination will be the only tools required to reach a correct diagnosis. Training in the identification of warning signs and symptoms, as well as the appropriate choice of diagnostic tests, will be key to accurate guidance. This article shows some of the neurological emergencies that we may encounter in our daily practice, such as syncope, altered level of consciousness, status epilepticus, acute hemiparesis, acute ataxia and acute hypotonia. |
| Resumen
Las urgencias neurológicas no son el motivo más frecuente de asistencia a los Servicios de Atención Primaria o Urgencias Pediátricas. En muchas ocasiones, en especial durante nuestra formación, pueden resultarnos difíciles de abordar, producirnos cierto rechazo y hacernos sentir inseguros en su manejo. Aplicar una evaluación sistemática en estos pacientes ayuda significativamente en su diagnóstico y tratamiento posterior. En la mayoría de las ocasiones, una historia clínica y una exploración física, completas y detalladas, serán las únicas herramientas que se necesiten para llegar a un diagnóstico adecuado. El entrenamiento en la identificación de signos y síntomas de alarma, así como la elección adecuada de pruebas diagnósticas, será clave para una orientación precisa. En este artículo se muestran algunas de las urgencias neurológicas que podemos encontrar en nuestra práctica diaria, como son: el síncope, la alteración del nivel de conciencia, el estatus epiléptico, la hemiparesia aguda, la ataxia aguda y la hipotonía aguda. |
Key words: Syncope; Status; Hemiparesis; Ataxia; Hypotonia.
Palabras clave: Síncope; Estatus; Hemiparesia; Ataxia; Hipotonía.
Pediatr Integral 2024; XXVIII (2): 79 – 94
OBJECTIVES
• To recognize the most frequent neurological emergencies in Pediatrics.
• To detect the factors that imply severity in syncope and altered level of consciousness.
• To delve into the therapeutic approach to status epilepticus.
• To understand the concept of “stroke mimics” and know the main clinical entities.
• To select the appropriate complementary tests based on the etiological suspicion of acute ataxia.
• To learn the main clinical conditions causing acute hypotonia.
|
|
|


Neurological emergencies in Pediatrics
Introduction
Neurological emergencies are not the most frequent reason for attending Primary Care or Pediatric Emergency Services. Training in the identification of warning signs and symptoms, as well as the appropriate choice of diagnostic tests, will be key to accurate guidance. This article shows some of the neurological emergencies that we can encounter in our daily practice, such as: syncope, altered level of consciousness, status epilepticus, acute hemiparesis, acute ataxia and acute hypotonia.
Syncope
The diagnosis of syncope depends on an adequate history and examination. Understanding the mechanisms of syncope helps with correct interpretation and minimizes diagnostic errors.
Definitions
Syncope is defined as a sudden, brief loss of consciousness and postural tone with spontaneous recovery. Presyncope refers to prodromal presentation without loss of consciousness.
Etiology
The etiologies associated with syncope in the pediatric population vary from autonomic/neurogenic dysfunction to hypertrophic cardiomyopathy and seizure disorders(1). Autonomic forms, especially vasovagal syncope, comprise up to 80%(2). Potentially serious etiologies are relatively rare, but require diagnostic consideration in the event of warning signs or symptoms (Fig. 1).

Figure 1. Causes and warning signs of potentially severe syncope. Adapted from: Callahan JM. 2015.
Classification
• Reflex syncope, neuromediated or autonomic:
– Vasovagal syncope: it is the most common. It is due to cardiovascular autonomic dysregulation that leads to sudden and transient cerebral hypoperfusion. It is associated with emotional stress (fear, pain, vision of blood) or orthostatic stress (getting up quickly, standing for a long time, hot environment)(2). The presence of triggering factors such as: standing, environmental heat, intense emotions or prodromes with vegetative symptoms, followed by loss of consciousness lasting seconds with rapid recovery, point, in a healthy patient with no history of interest, to vasovagal syncope. Muscle jerks (tonic spasms or myoclonus) may appear if cerebral hypoperfusion is prolonged (convulsive syncope).
– Situational: similar to vasovagal syncope but with a specific trigger. In the context of coughing/sneezing, combing, urination, carotid sinus pressure, etc.
– Febrile syncope: many hypotonic febrile seizures or only with loss of consciousness could be febrile syncope. Performing an electrocardiogram (ECG) in these patients is recommended, since it may be the initial presentation of arrhythmogenic heart disease.
– Syncope due to orthostatic hypotension: due to autonomic dysfunction in vasoconstriction. The feeling of dizziness or “orthostatism” may appear when standing up quickly on multiple occasions, even without syncope occurring.
– Postural orthostatic tachycardia syncope: there is an increase in heart rate of 30-35 beats per minute upon standing along with prodromes similar to vasovagal syncope, which may be associated with a sensation of palpitations. Patients report intolerance to standing.
• Cardiogenic syncope: related to arrhythmogenic or structural cardiac pathology. A personal history of congenital or acquired heart disease with residual cardiac dysfunction or arrhythmia, syncope while lying down or with effort, the presence of pathological murmurs, signs of heart failure or rhythm abnormalities will point towards cardiac pathology.
• Epileptic seizure/convulsion: in those epileptic seizures that could be confused with vasovagal syncope, the loss of consciousness is usually of longer duration, the associated movements appear in the first moments of the episode and the recovery is longer, with postictal confusion or other neurological symptoms appearing.
• Functional disorder: the episodes occur in front of witnesses, they may appear “theatrical” (eye movements, sighs, etc.) and injuries do not usually occur with the fall, since self-protection behaviors are preserved.
• Others: sobbing spasms, metabolic syncope, basilar migraine, subarachnoid hemorrhage, etc.
Approach in the Emergency Room
Assessment
The goal of syncope evaluation is to identify potentially severe conditions. An initial study for pediatric patients with syncope includes(3):
• Full history to identify previous events or triggering factors, and collect a description of the event that includes previous symptoms (prodromes) and recovery from the episode. Personal and family history of interest should be collected, especially the history of complex heart disease, sudden death at a young age, and sensorineural hearing loss.
• Complete physical examination, including orthostatic vital signs (blood pressure and heart rate), complete cardiac examination and complete neurological examination.
• ECG, a simple and non-invasive test that can be performed at the bedside. Particular attention should be paid to signs of hypertrophy or abnormal conduction times (e.g., long QT syndrome) or ST changes (e.g., Brugada syndrome).
Other studies:
• Capillary blood glucose: if no recovery at the time of evaluation, if prolonged fasting or at-risk patients (e.g., hypoglycemic treatments).
• EEG in its different varieties: indicated if an epileptic seizure is suspected, not as a routine.
Treatment
Initial stabilization will be a priority at the time of syncope. Subsequently, action will be taken based on the etiology that caused it.
The most effective treatment for autonomic and orthostatic causes of syncope is to ensure adequate fluid intake and avoid fasting. Small amounts of salty foods can also help maintain intravascular volume(3). It is advisable to train patients to lie down when they have prodromal symptoms to prevent syncope.
Referral for study
Patients with: cardiovascular disease or an abnormal cardiac examination, severe ECG abnormalities (e.g., prolonged QTc interval or complete heart blocks), syncope with chest pain or cyanotic episodes, apnea or focal neurological findings, toxic ingestion or orthostatic hypotension that does not respond to intravenous fluids(3,4). All patients with signs or symptoms of potentially severe syncope should be referred to Cardiology (Fig. 1)(3). Referral should be made to Neurology in the event of focal neurological findings, other neurological anomalies or a history suggestive of epilepsy/seizure(3,4).
Altered level of consciousness
An altered level of consciousness represents an emergency situation where early initial stabilization aimed at maintaining cardiorespiratory functions and avoiding neurological deterioration is essential.
Definitions
Consciousness is the physiological process through which the individual maintains a state of alert with full knowledge of himself and his environment. It relies on the functional and anatomical integrity of two structures: the cerebral cortex and the ascending reticular activating system (ARAS), which starts from the brain stem and projects to the cerebral cortex. Therefore, alterations in the level of consciousness originate from structural or functional dysfunction of the ARAS or at the cortico-subcortical level(5).
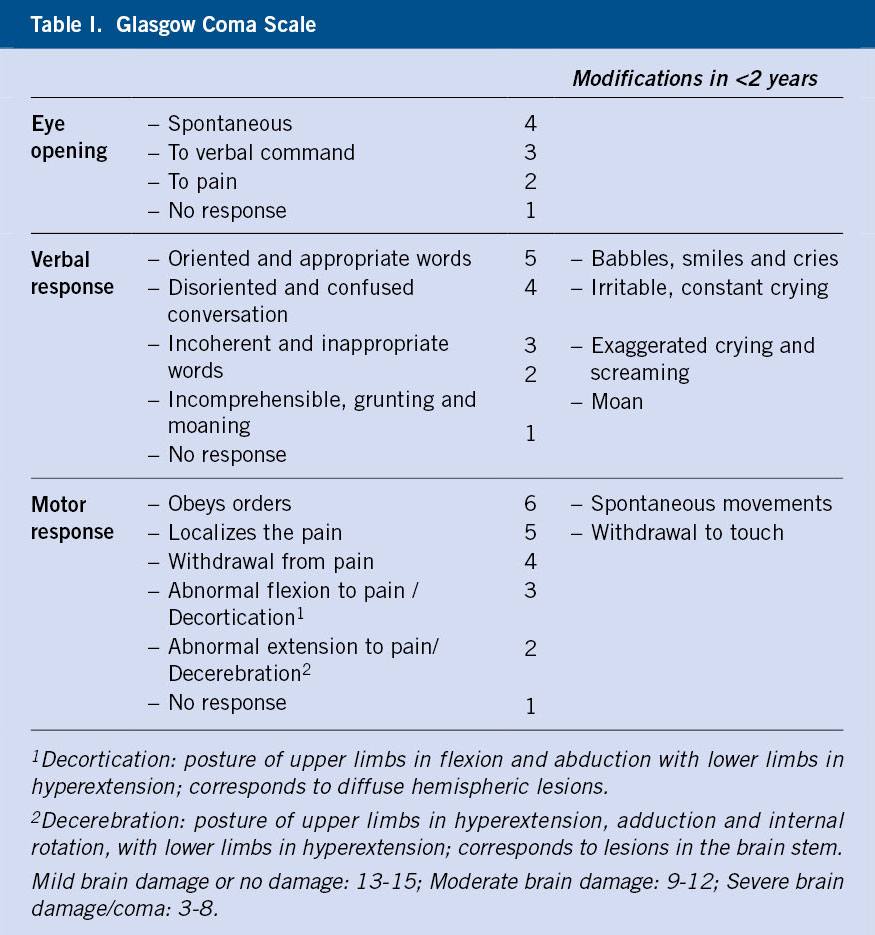
There is a spectrum of altered consciousness between full alertness and coma. Coma is the deepest degree of altered consciousness with lack of response to stimuli. Terms such as drowsiness, stupor, obtundation and lethargy should be avoided due to their subjectivity(6). Instead, there are objective scales to quantify the severity of coma, such as the Glasgow Coma Scale (GCS), which consists of the evaluation of ocular, verbal and motor responses. The state of consciousness is determined by adding the maximum value obtained in each section, which ranges between 3 and 15 (Table I)(7,8).
Etiology
The most frequent causes of altered level of consciousness in the pediatric population are: infections of the central nervous system (CNS), severe systemic infections, traumatic brain injury (TBI), hypoglycemia, poisoning, seizures and post-critical states(6,9). The most frequent causes are presented below, divided according to their etiology.
• Primary brain alteration or structural alteration. Alteration in the level of consciousness, usually of rapid onset, with neurological focality and/or asymmetries in the physical examination.
– CNS infection: encephalitis, meningitis, abscess.
– TBI and diffuse axonal injury.
– CNS tumors.
– Vascular: hemorrhage (arteriovenous malformations, aneurysms, coagulopathy…) or ischemia (venous sinus thrombosis, thromboembolism…).
– Non-convulsive status and postcritical state.
– Hypoxic ischemic encephalopathy.
– Hydrocephalus.
• Toxic-metabolic alteration. It usually has a progressive and fluctuating onset, normally without focality or asymmetries in the examination.
– Exogenous factors: toxics, drugs and medicines.
– Endogenous factors: severe systemic infection, hypo/hyperglycemia, ionic alterations, diabetic ketoacidosis, decompensation of metabolic diseases, etc.
Approach in the Emergency Room
Initial stabilization measures must be carried out early in any patient with an altered level of consciousness, without any of the complementary tests delaying them(6). Subsequently or while stabilization is being carried out, the history, physical examination and complementary tests aimed at identifying the cause will be carried out.
In the physical examination, some aspects are of special interest, such as:
• Pupils: alterations in reactivity, symmetry and/or size of the pupils may indicate structural lesions or toxic-metabolic etiologies.
• Eye movements: these include oculocephalic reflex (OCR, “doll eyes”) and oculovestibular (OVR). Both are equivalent and their presence indicates integrity of the midbrain, pons, and oculomotor nerves in a comatose patient. The OCR explores the conjugate deviation of the gaze in the opposite direction to the passive mobilization of the head, both vertically and horizontally. The OVR is produced after the instillation of cold water into the external auditory canal, and explores ocular deviation towards that ear, with compensatory nystagmus.
• Fundus of the eye: the presence of papilledema may indicate intracranial hypertension (ICH). Retinal hemorrhage may indicate intracranial hemorrhage.
Complementary tests will be guided based on the findings of the examination and history, but the majority of patients with altered level of consciousness will require a complete blood and urine analysis, which includes detection of toxic substances, in addition to an ECG and a neuroimaging test. There is no neuroimaging of choice for the patient with altered level of consciousness, since this will depend on technical availability, the patient’s characteristics and the diagnostic approach(6) (Fig. 2).

Figure 2. Proposal for addressing the alteration of the level of consciousness in the Emergency Room. BP: blood pressure; CRP: C-reactive protein; CT: computed tomography; FH: family history; ECG: electrocardiogram; EEG: electroencephalogram; F-US: fontanelle ultrasound; GCS: Glasgow Coma Scale; HR: heart rate; ICP: intracranial pressure; MRI: magnetic resonance imaging; OCR: oculocephalic reflex; OTI: orotracheal intubation; OVR: oculovestibular reflex; PH: personal history; RR: respiratory rate; SE: status epilepticus; T: temperature; TBI: traumatic brain injury.
Treatment
The cornerstone of treatment will be initial stabilization, which includes measures and procedures aimed at maintaining respiratory and cardiocirculatory functions. It is also essential to urgently treat situations that may imply rapid neurological deterioration, such as the presence or suspicion of ICH. Measures to reduce ICH include: intubation and hyperventilation, sedation, elevation of the patient’s head and specific treatments, such as mannitol or hypertonic saline.
Etiological treatment will be essential to achieve full recovery, but in many cases, it cannot be carried out immediately until the results of complementary tests are available. Specific empirical treatments can be considered depending on the suspicion:
• Naloxone: miosis, respiratory depression, and/or evidence of opioid use.
• Flumazenil: suspected benzodiazepine poisoning.
• Activated charcoal: consider if drug overdose is suspected, as long as the airway is protected.
• Empirical antibiotic therapy and/or acyclovir: suspected sepsis or CNS infection.
Status epilepticus
Status epilepticus is the most common neurological emergency in pediatric patients. Early treatment with benzodiazepines is essential to end the seizure and reduce possible sequelae.
Definition
Status epilepticus (SE) is defined as an abnormally prolonged seizure that can cause long-term sequelae(10). It is due to the failure of the mechanisms responsible for ending the seizure; therefore, it typically does not resolve without medical intervention(10,11). The definition of SE has been debated over the years. Thus, from the classic concept of seizures lasting more than 30 minutes or repeated seizures without complete recovery between them, it has evolved to a current definition of greater complexity, which creates 3 main categories(10,12) (Fig. 3):

Figure 3. Categories of status epilepticus.
• Early SE: epileptic seizure that lasts beyond the so-called time 1 (T1), after which it is unlikely that the seizure will end on its own. The duration of T1 varies depending on the type of seizure, between 5 minutes for a normal seizure generalized tonic-clonic seizure (GTCS) and the 10 minutes for focal or absence seizures. It is essential to start antiepileptic treatment to try to reduce the morbidity and mortality associated with SE.
• Established SE: it continues despite the administration of first-line drugs at correct doses, usually more than 10-30 minutes.
• Refractory SE: persistence of the seizure despite treatment with two different antiepileptic drugs at adequate doses, exceeding time 2 (T2), after which there is a high risk of long-term sequelae. The duration of T2 also varies between 30 minutes for GTCS, 60 minutes for focal and unknown in the case of absence seizures. The risk of severe complications requires more intensive treatment(11). Within the refractory SE, there are:
– Super-refractory SE, if the duration is greater than 24 hours.
– New-onset refractory status epilepticus (NORSE), which occurs in a patient without a history of epilepsy or other known or evident previous neurological pathology(13).
– FIRES syndrome (febrile infection-related epilepsy syndrome), a subtype of NORSE that follows a febrile episode that occurs between 2 weeks and 24 hours before the onset of the seizure(12,13).
Classification
Currently, multiple classifications are used based on four different variables: seizure semiology, etiology, electroencephalographic (EEG) findings, and patient age. An attempt should be made to classify SE according to all the variables, taking into account that it is a dynamic process, since both the seizure semiology and the EEG pattern can vary(11,12) (Table II).

Epidemiology
SE is the most common neurological emergency in children(10-12,14), with high morbidity and mortality and a high probability of neurological sequelae(12). The incidence ranges between 4 and 58 per 100,000 inhabitants per year in the pediatric population(10-12). The highest incidence is observed in children under 2 years of age, probably due to a higher rate of symptomatic causes or a greater susceptibility due to brain immaturity(11). Up to 20-25% of patients with epilepsy will present at least one SE, with 10% of them being the first form of their epilepsy(12). The incidence of refractory SE ranges between 10 and 40% of SE, while super-refractory SE represents up to 10%(12).
Prognosis
The morbidity derived from a SE is high. There is more than a 15% probability of long-term neurological sequelae, such as motor deficits, intellectual disability or behavioral disorders(11,12). Approximately 20% will present at least one other SE, especially in the first year and in children with underlying neurological pathology(11). The probability of developing epilepsy after an SE reaches 25% in previously healthy children and 46% in children with neurological disorders(11). Short-term mortality is 3-5% and is mainly due to acute complications (respiratory failure, metabolic acidosis, intracranial hypertension, etc.), although it must be taken into account that the main cause of SE in children is febrile, whose estimated mortality is 0.2%(11,12).
Diagnosis
The following will be essential: a thorough medical history and a detailed physical examination(11). The former will include: possible history of trauma, infection, metabolic alteration or exposure to toxins, as well as the semiological characteristics of the seizure(11,12). In patients with known epilepsy, possible precipitating factors of decompensation should be investigated, such as: lack of adherence to treatment, intercurrent infectious process, diarrhea, vomiting, etc.(11). Complementary tests will be indicated in most processes, and will be fundamentally oriented towards the search for reversible causes(11,12,14) (Table III).

Treatment
Its objective, in addition to ending the seizure as early as possible to avoid sequelae, is to maintain vital functions and try to detect treatable and/or potentially more serious causes(12,14). Most clinical guidelines propose a stepwise treatment based on the time of evolution(12,15). The doses of each drug, as well as their main adverse effects, are shown in table IV. An algorithm is proposed in figure 4.


Figure 4. Treatment algorithm proposal of status epilepticus (SE). BRV: brivaracetam; BZD: benzodiazepines; CI: continuous infusion; CNZ: clonazepam; DZP: diazepam; GCS: Glasgow Coma Scale; IVIG: intravenous immunoglobulins; LEV: levetiracetam; LCS: lacosamide; MDZ: midazolam; OTI: orotracheal intubation; PB: phenobarbital; PER: perampanel; PHT: phenytoin; SE: status epilepticus; TPM: topiramate; VPA: valproic acid.
• General measures. The first step in the management of SE is, as in any medical emergency, to secure the airway and maintain adequate oxygenation and ventilation. Continuous monitoring of vital signs and peripheral venous access should be initiated early, to detect possible analytical alterations (hypoglycemia, alterations in blood pH, etc.) and to be able to establish intravenous treatment early (antiepileptics, fluid therapy, vasoactive drugs, etc.)(11,12,14).
• First-line treatment (active crisis, early SE). Benzodiazepines (BZD) constitute the first-line antiepileptic treatment due to their speed of action, their wide range of presentations, in addition to the intravenous one since they manage to jugulate up to 80% of prolonged seizures(11,12,14). For these reasons, the prevention of SE must include rescue antiepileptic medication to be administered by the main caregivers, who must be adequately instructed in its management(10). The most commonly used rescue antiepileptic medication options are rectal diazepam (Stesolid®) and oral midazolam (Buccolam®, Oroxelam®)(11,16). The mechanism of action of BZDs is to enhance the effect of GABA, the main inhibitory neurotransmitter. The most common side effects are: respiratory depression and arterial hypotension, although they are rare at adequate doses. It is recommended to administer between 1 and 2 full doses of BZD early to optimize its effectiveness without significant risk of side effects(12,15).
• Second line treatment (established SE). It should begin between 10 and 15 minutes after the onset of the seizure, when BZD treatment has failed. There is currently no clearly superior drug, so its choice must be individualized according to the type of SE, the patient’s conditions and the possible side effects(11,12).
• Third and fourth line treatment (refractory and super-refractory SE). Anesthetic drugs are used (BZD, thiopental, propofol, ketamine) whose objective will be induced coma, which should be maintained for 24-48 hours, during which future maintenance antiepileptic treatment will begin. Due to the complexity of this situation, management will ideally be carried out in a Pediatric Intensive Care unit. If SE persists for more than 24 hours or if it reappears after medication is withdrawn, 2nd and 3rd line drugs that have not been used previously should be used or different antiepileptic drugs and other options should be considered, such as: ketogenic diet, immunomodulatory treatment or epilepsy surgery.
Acute hemiparesis/stroke
Recognition and differential diagnosis of acute hemiparesis is challenging, particularly at early ages. Clinical findings combined with neuroimaging are essential for diagnosis and treatment.
Definition
The onset of acute hemiparesis/hemiplegia in a pediatric patient is always worrying. Although the etiology is diverse, cerebral stroke must be included in the differential diagnosis, quickly activating all the protocols established in our environment.
Correct clinical identification of acute hemiparesis avoids unnecessary diagnostic or therapeutic procedures and allows the early implementation of specific therapeutic measures for each etiology, some of them severe.
Etiology
Cerebrovascular accident/stroke
We can distinguish between ischemic stroke (arterial or venous) and hemorrhagic stroke. The underlying risk factors are diverse, such as: focal cerebral arteriopathy, arterial dissection, structural heart disease, sickle cell anemia or arteriovenous malformation, among many other causes. Arterial ischemic strokes most commonly present with a focal neurological deficit, such as hemiparesis, which is the most common focal manifestation. Hemorrhagic strokes present more frequently with headache or altered mental status compared with ischemic arterial strokes. Epileptic seizures can occur in all types.
Stroke mimics
These are entities that are difficult to clinically differentiate from stroke. They must be taken into account due to their frequency and because some are serious neurological pathologies that require urgent diagnosis and treatment. Among them are: hemiplegic migraine, Todd’s paralysis, acute disseminated encephalomyelitis (ADEM), alternating hemiplegia, brain tumors, CNS infections, stroke-like in mitochondrial diseases, hypoglycemia, psychogenic symptoms and poisoning(17). Table V shows the characteristics of some stroke simulators.
The gradual and progressive spread of one aura symptom after another, the presence of positive symptoms, such as visual flashes or paresthesias, or the association with nausea, vomiting, photophobia and phonophobia, is suggestive of migraine.
The presence of previous paroxysmal symptoms, such as muscle contractions, cephalic version or loss of consciousness, together with the recovery of hemiparesis in a short period of time, should make us suspect an epileptic seizure.
The presence of clinical findings inconsistent with neurological pathology, during the clinical history or examination, may be related to a functional etiology.
Approach in the Emergency
Room
Assessment
• Clinical history and physical examination: precision in the initial evaluation of the patient is a fundamental tool in the differential diagnosis of acute hemiparesis (Algorithm 1). Family history of similar conditions, previous high-risk diseases (congenital heart disease, sickle cell anemia, arthropathies), use of drugs, progression and duration of hemiparesis, accompanying and preceding symptoms must be evaluated in detail. The neurological examination must be complete, paying special attention to the location of the lesion, evaluation of the level of consciousness and the progression over time of the signs and symptoms. The pediatric examination should not overlook the identification of signs of infection, as well as a complete cardiological examination with blood pressure measurement.
• Neuroimaging: urgent neuroimaging will be necessary in case of suspected recent onset hemiparesis.
Magnetic resonance imaging (MRI), if possible MRI angiography, is preferred for the differential diagnosis. It has better temporal, spatial and diagnostic resolution, but it is unlikely to be available on an emergency basis(18). Rapid protocols that prioritize diffusion-weighted images(19) are very useful in the first hours to differentiate a stroke from its simulators.
Cranial computed tomography (CT) allows for studies to be performed in a short time and to quickly identify cranial hemorrhages or tumors, but may be normal in the first hours of the ischemic stroke. In the case of suspected ischemic stroke, perfusion CT and CT angiography can improve detection, identify large vessel occlusion, and estimate the core of the infarct and the penumbra area. These are studies with a higher radiation rate than the conventional technique, which should be requested only in cases of high suspicion of stroke, if urgent MRI is not available.
• Additional studies(18): it is advisable to perform a blood test that includes full blood count and biochemistry with: blood glucose, ions, liver function, kidney function, clotting, lactic acid and markers of infection. Blood or CSF analytical studies can help in the differential diagnosis, for example, of infectious and metabolic processes (MELAS), among others.
A lumbar puncture would be indicated: when there are no contraindications, if there are signs of infection, autoinflammatory/autoimmune disorders, metabolic disease or suspected subarachnoid hemorrhage not confirmed by imaging.
Treatment
Initial stabilization is a priority in a patient with acute hemiparesis. These patients require admission to the PICU. Neuroprotective measures, such as maintaining homeostasis, adequate ventilation and oxygenation, or avoiding hypotension, among others, should be started as soon as possible.
The specific treatment will depend on the defined cause:
• Pediatric stroke: treatment is based on brain protection, assessment of revascularization techniques/reperfusion, treatment of sequelae and triggering factors. Specific treatment will depend on the type of stroke, the presence of brain hemorrhage, and other individual factors. Reperfusion therapies could be applied in selected pediatric patients with ischemic stroke in the first hours, both with tissue plasminogen activator (tPA) and thrombectomy. It will be necessary to know the existence, or not, of a “Pediatric Stroke Code” in our environment, in order to reduce the time of diagnosis and treatment of these patients. In all cases, it is essential to: maintain adequate ventilation and oxygenation, normoglycemia, normothermia, avoid hypotension and epileptic seizures(17). It is recommended to start early preventive treatment to avoid recurrences, with anticoagulants (low molecular weight heparin or unfractionated heparin) or antiplatelet agents (aspirin).
• Hemiplegic migraine: in the acute episode, symptomatic treatment of the headache and accompanying symptoms is recommended. The use of triptans is controversial. In severe cases, parenteral corticosteroids may be used. As preventive treatment, the same drugs as for other migraines could be used. Verapamil has been recommended in those patients with many auras. Acetazolamide has been used in patients with familial hemiplegic migraine.
• Alternating hemiplegia: Flunarizine is the drug most commonly used to reduce the frequency and intensity of episodes.
• Epileptic seizures: the rescue treatment for epileptic seizures continues to be benzodiazepines (diazepam, midazolam). If it is epilepsy, the maintenance antiepileptic drug should be chosen based on the characteristics of the patient and the type of epilepsy.
• Acute Disseminated Encephalomyelitis (ADEM): the mainstay of treatment is high-dose intravenous glucocorticoids. Other options are intravenous immunoglobulins and plasmapheresis.
• Mitochondrial encephalopathy, lactic acidosis and “stroke-like” episodes (MELAS): Arginine supplementation has been used to treat acute episodes and as maintenance. Epileptic seizures must be treated vigorously. The use of urgent intravenous saline with dextrose is recommended to maintain energy supply and cerebral perfusion during an acute episode.
Prognosis
Initiating adequate treatment in the shortest possible time is essential in the face of acute hemiparesis, being one of the factors most closely related to prognosis. Any intervention to improve outcomes, such as applying neuroprotective measures from the beginning, could benefit the patient throughout their life(20).
In the case of stroke in Pediatrics, approximately 75% of patients suffer long-term neurological morbidity(21). Reducing the time of care and treatment of these patients will favor their optimal long-term prognosis.
Acute ataxia
Although acute ataxia in pediatric age is frequently due to poisoning or self-limited post-infectious symptoms, the identification and treatment of other potentially serious causes should be as early as possible. There is a time limit after which recovery of established cerebellar damage is not possible.
Definition
Ataxia refers to alterations in the coordination of posture and movement. Acute ataxia is one with a duration of less than 72 hours. Some authors include a duration of less than 7 days.
Pathophysiology of ataxia(22)
The origin of ataxia is related to the alteration of the structures that regulate balance and coordination.
• Cerebellar origin: damage isolated to the cerebellum or in combination with other connected brain structures, such as the brainstem. It is divided into: kinetic or hemispheric ataxia (dysmetria, dysdiadochokinesia, tremor), static or vermian ataxia (truncal ataxia, increased base of support) and global ataxia. Nystagmus is multidirectional and Romberg test is negative.
• Vestibular origin: associated with dysfunction of the vestibular system. It is characterized by unstable gait with inclination/deviation of the postural axis and associated sensation of vertigo. Horizontal nystagmus and positive Romberg test with a latency period are observed.
• Sensory origin: involvement of the proprioception due to damage to the posterior spinal cords or peripheral sensory nerves. Walking is unsafe with sudden corrections and may be accompanied by paresthesias. There is hyporeflexia and Romberg test is positive. It is the ataxia that can be associated with Guillain-Barré syndrome.
Approach in the Emergency Room
Clinical history
The following should be inquired: time of evolution, recent infections or vaccinations, symptoms of current infection, accompanying symptoms and their progression. One should ask about the possibility of access to toxic substances or head trauma, as well as personal and family history.
Physical exploration
It must be general, including taking constants. During the neurological examination, special attention should be paid to focal neurologic deficit, level of consciousness and signs of intracranial hypertension or nervous system infection. Regarding the ataxia itself, assess:
• Alteration of posture and gait(23). Imbalance, increased base of support, inability to walk or sit. Some maneuvers are useful, such as the Romberg test (it especially evaluates proprioception) or the Barany test, in which the patient remains seated with eyes closed and arms extended in front, which should not deviate (it especially evaluates the vestibular system).
• Alteration of limb movement. The following should be highlighted:
– Dysmetria. Inability to reach objects with hands, arms or legs. It is examined using index-nose and heel-knee tests.
– Action and postural tremor. The patient will pour water from one glass to another.
– Dysdiadochokinesia. Inability to synchronous alternating movements. It is explored by using the hand movement of screwing in a light bulb or alternately tapping the palm/back of the hands on the thighs.
• Language alteration. It includes mutism and dysarthria with slow, explosive, and often nasal speech.
• Alteration of muscle tone. Hypotonia, especially after acute cerebellar injury.
• Oculomotor alterations. Fixation and pursuit deficits, nystagmus, alignment disorder, oculomotor apraxia, etc.
• Cognitive alteration. Abnormality of executive functions and visuospatial disorders, inability to read and write, and inappropriate behaviors. There may be problems with: attention, perseveration, impulsivity, anhedonia and passivity.
• Emotional alterations.
Some data suggestive of severe neurological pathology in acute ataxia are: age over 5 years, presence of hypo/areflexia, dysmetria, alteration of consciousness or visual alteration (diplopia, papilledema, decreased visual field)(24).
Complementary tests
Urgent neuroimaging will be performed in: ataxia with altered level of consciousness, signs of intracranial hypertension, neurological focality, asymmetry of ataxia or history of head trauma(25). Patients under 5 years of age with previous viral infection, without signs or symptoms of extracerebellar involvement, can be managed without lumbar puncture or neuroimaging(25).
Approach in the Emergency Room according to etiology
Among the multiple causes of ataxia, infectious or parainfectious etiology is the most common. A global approach in the Emergency Department can be found in algorithm 2.
• Postinfectious acute cerebellar ataxia(26). It is the most common cause of ataxia. It affects patients aged 1-6 years and is an autoimmune reaction to a viral or bacterial infection. The agents that have been most related are: Varicella-zoster, Epstein-Barr, Coxackie, Echovirus, Enterovirus, Parvovirus, Mycoplasma pneumoniae and Borrelia burgdorferi. A few days or weeks after an infection, truncal ataxia, difficulties standing and intention tremor appear. Complementary tests are normal. The prognosis is favorable, without requiring treatment given its self-limiting nature.
• Acute cerebellitis. Similar to the previous clinical picture, but also associating: affectation of general condition, fever, vomiting, headache, photophobia and/or altered level of consciousness. There is elevation of acute phase reactants and pleocytosis or hyperproteinorrachia in CSF. Cranial MRI shows cerebellar edema, either global or focal. The treatment is etiological, of the infection. The effectiveness of corticosteroids is doubtful. Despite its severity, with appropriate treatment, the prognosis is favorable in the majority of cases.
• Cerebellar abscess. Generally due to extension of an ENT infection. It manifests with: fever, headache and cerebellar ataxia. The treatment is etiological for the infection, and may require neurosurgical treatment.
• Rhombencephalitis. Rare infection, associated with Listeria, Varicella-zoster or Enterovirus 71. It manifests as febrile ataxia and meningism. In CSF there may be pleocytosis and, in cranial MRI, involvement of the trunk and cerebellum.
• Opsoclonus-myoclonus-ataxia syndrome. It mainly appears in children under 4 years of age. It is an immune-mediated, paraneoplastic, parainfectious or idiopathic condition. Neuroblastoma is the neoplasm with which it is most related. Ataxia may be the first manifestation. It associates: myoclonus (sudden muscle contractions), opsoclonus (chaotic, brief and intermittent eye movement), irritability and sleep disturbances. Opsoclonus tends to be the later manifestation or may even be absent. Immunomodulatory treatment, for example, with corticosteroids, immunoglobulins and/or rituximab, has substantially improved the prognosis of patients. Untreated or undertreated patients usually present neurodevelopmental and behavioral sequelae.
• Miller-Fisher Syndrome(27). Variant of Guillain-Barré syndrome, which presents with the triad ataxia, areflexia and ophthalmoplegia. Hyperproteinorrachia may be found. Treatment is based on the use of immunoglobulins or plasmapheresis. The outcome is usually favorable with optimal recovery after 6 months.
• Acute disseminated encephalomyelitis (ADEM). Rare acute demyelinating disease that affects the brain, spinal cord and/or optic nerves, after a previous infectious condition. Neurological manifestations include: pyramidal signs, hemiparesis, ataxia, cranial nerve palsies, seizures and encephalopathy. The MRI shows demyelinating lesions. Treatment is based on high-dose corticosteroids, immunoglobulins and/or plasmapheresis. Although there may be catastrophic forms, the overall outcome is favorable in most cases.
• Acute labyrinthitis. Probably of viral origin, with ataxia, intense vertigo and nystagmus. Treatment with corticosteroids is useful.
• Neoplasms. Ataxia can appear as a symptom in tumors of the cerebellum, brain, pons, and spinal cord.
• Post-concussion syndrome. After head or neck trauma. It associates headache, vomiting and confusion.
• Cerebellar stroke. The most frequent clinical manifestations are: ataxia, vertigo, vomiting and headache. It is confirmed by neuroimaging. Neurosurgical treatment may be required in cases with hemorrhage or large edema, for decompression.
• Toxic-metabolic. Ataxia may appear in the context of metabolic abnormalities, such as hypoglycemia, hyponatremia and hyperammonemia. Also, due to accidental or provoked ingestion of toxic substances: alcohol, benzodiazepines, opioids, antihistamines, antiepileptics, among others.
• Functional disorder. Inconsistencies are found in the examination.
Acute hypotonia
Hypotonia can appear acutely as a sign of multiple systemic disorders. The accompanying symptoms will be essential to properly guide the diagnosis.
Definition
Hypotonia is defined as the decrease in the resistance of the muscles to passive stretching, compared to weakness, which is the decrease in the maximum force that can be generated voluntarily. Hypotonia can arise from injury to any region of the nervous system or be influenced by other circumstances, such as stress or visceral pain. Hypotonia may occur with or without weakness; whereas weakness always implies hypotonia. This article focuses on entities with an acute onset, so those with a chronic course, such as spinal muscular atrophy, will not be addressed.
Classification(28)
Depending on the location of the lesion, it has traditionally been divided into hypotonia of central and peripheral origin, with symptoms corresponding to first and second motor neuron lesions, respectively. However, sometimes it is not easy to make this distinction, due to overlapping characteristics of both conditions (mixed hypotonia).
• Central hypotonia. The most frequent. It occurs due to involvement of the central nervous system (CNS). Hypotonia will be predominantly axial, with preserved limb movements against gravity. Deep tendon reflexes (DTR) will be normal or elevated. There may be altered contact or level of consciousness and epileptic seizures. Neuroimaging may be altered. The main causes are:
– Acute encephalopathy. It includes: hypoxic-ischemic encephalopathy (the most common cause of acute neonatal hypotonia), cerebrovascular accidents, acute toxic-metabolic disorders and CNS infections. They require early detection and treatment to reduce sequelae.
– Chromosomopathies or genetic alterations. There are usually accompanying phenotypic features and hypotonia is chronic. Some examples are: trisomy 21, Prader-Willi syndrome, Williams syndrome, etc.
– Inborn errors of metabolism. Some present acutely after an asymptomatic period.
– Congenital anomalies of the CNS.
– Others. Trauma at the cranio-spinal level, heart failure or other systemic affections.
• Peripheral hypotonia(29). Involvement of the peripheral nervous system (PNS). Hypotonia will be global, both axial and distal, with associated muscle weakness(30). DTRs will be decreased or absent. There is no alteration in contact or level of consciousness and the neuroimaging is normal. It may be associated with: ventilation and swallowing disorders, elevation of muscle enzymes (CK), muscle atrophy and fasciculations. Depending on the location of the injury, the main causes are:
– Anterior horn motor neuron: spinal muscular atrophy, chronic course.
– Peripheral nerve: neuropathies, chronic course.
– Neuromuscular junction: myasthenic syndromes; some of them, such as myasthenia gravis or botulism, can be acute in onset.
– Muscle fiber: congenital myopathies and muscular dystrophies, of chronic course.
Physical examination
Any pediatric examination should include a basic neurological examination, in which muscle tone will be evaluated. Tone is examined in neonates or small infants using techniques such as ventral suspension, traction maneuver, vertical suspension, or the scarf sign. At later ages, it is explored through passive mobilization, grading from 1 to 4 using the Ashworth scale. Hypotonia must be differentiated from hyperelasticity or increased range of motion of a joint without hypotony. Strength is examined through the ability to maintain antigravity posture of limbs or the response to resistance. Fatiguability is explored by repeating movements (opening and closing hands) or maintaining a posture for a few minutes (looking up).
Approach based on etiology
• Acute myelitis(31). It is a neuroinflammatory condition of the spinal cord. In relation to viral (enterovirus) or autoimmune processes. After a febrile process, hours or days later, a picture of flaccid paralysis, hypotonia and areflexia begins, with an asymmetric distribution. The most important complication is respiratory failure and dysautonomia. The MRI is altered, with increased T2 signal in the gray matter of the spinal cord, whether or not associated with increased signal from nerve roots. Pleocytosis is usually present in the CSF. In addition to CSF cultures and serologies, pharyngeal and rectal swabs should be requested to rule out viruses. The diagnosis is made by imaging and microbiological confirmation. Treatment is supportive, along with corticosteroids.
• Guillain-Barré syndrome(32). It is the most common cause of acute neuromuscular weakness. Its etiology is autoimmune, after infections by Campylobacter jejuni, Cytomegalovirus, Mycoplasma pneumoniae or Influenza virus. It generally begins with distal and symmetrical paresthesias, followed by ascending weakness with rapid progression. There are atypical forms, starting in the upper extremities or facial muscles. Hyperproteinorrachia may appear in CSF. The electroneurogram (ENG) shows slowing of conduction velocity. Treatment is carried out with immunoglobulins or plasmapheresis. The outcome is usually favorable in weeks-months. 10-20% will present persistent motor deficits.
• Childhood/juvenile myasthenia gravis. It is an autoimmune condition due to anti-acetylcholine (ACh) receptor antibodies, among others. It can be associated with other autoimmune diseases, such as Hashimoto’s disease or autoimmune polymyositis. The initial manifestation is usually: ptosis, strabismus and diplopia, but the pupils are usually not affected. In adolescents it is more common for it to evolve into a generalized form, with hypotonia and global fatigue. There is a life-threatening risk due to the involvement of the respiratory muscles. It is important to demonstrate fatigue for the diagnosis. Complementary tests include: serological tests to identify antibodies; pharmacological test with edrophonium, an acetyl-cholinesterase (AChE) inhibitor drug that temporarily improves symptoms, which will be carried out in a hospital environment; and electrophysiological test (ENG). Treatment is with pyridostigmine, an AChE inhibitor. In generalized forms, immunosuppressants must be combined. Thymectomy is not an intervention of choice in the pediatric age, except in cases of resistance to conventional treatment.
• Botulism(33,34). It is due to exposure to Clostridium botulinum (CB) toxin through ingestion of contaminated food, through wounds or by inhalation. The following are considered risky environments: rural areas, construction areas, exposure to dust or contact with animals. The toxin produces a blockade of the presynaptic release of ACh at the neuromuscular junction. It causes mydriasis and progressive descending flaccid paralysis, which can lead to respiratory failure. Affectation in infants is rare. There are mild forms, with poor crying, hypoactivity and constipation. The diagnosis consists of identifying the toxin in feces and/or blood or identifying the pathogen in the digestive tract. Treatment requires stabilization and support measures. In severe cases, botulinum antitoxin of equine origin or specific human immunoglobulin can be used. The prognosis is favorable, generally, with full recovery within several weeks and a mortality rate of less than 1%.
Role of the Primary Care pediatrician
If a pediatric patient presents to the Primary Care clinic with a neurological emergency, the pediatrician’s role should focus on initial stabilization and early out-of-hospital treatment, such as in epileptic seizures. In addition, the Primary Care pediatrician is a fundamental figure for the activation of emergency/transportation services and the coordination with hospital services, when transfer is necessary.
In cases where the patient arrives stable or the event has resolved, the pediatrician will assume the main role in the approach and diagnosis of patients, referring only necessary cases to hospital specialists.
Conflict of interests
There is no conflict of interest in the preparation of the manuscript. Declaration of interests: none.
Bibliography
The asterisks show the interest of the article in the authors’ opinion.
1. Zhang O, Du J, Wang C, Du Z, Wang L, Tang C. The diagnostic protocol in children and adolescents with Syncope: a multi-center prospective study. Paediatr Act. 2009; 98: 879-84.
2. Bonilla L, Daghoum D. Síncope. Espasmo del sollozo. Spasm of sobbing. In: Benito J, Mintegi S. Urgencias Pediátricas. 2nd Pan-American Ed; 2019. p. 980-5.
3. Callahan JM. Syncope. In: Selbst SM. Pediatric Emergency Medicine Secrets. 3th Third Ed. Elsevier – Health Sciences Division; 2015. p. 184-9.
4. Massin MM, Bourguignont A, Coremans C, Comté L, Lepage P, Gérard P. Syncope in pediatric patients presenting to an emergency department. J Pediatr. 2004; 145: 223-8.
5. Zeman A. Consciousness. Brain. 2001; 124: 1263-89.
6. Cambra F, Lasuen N, Palomeque A. Coma: etiología, fisiopatología y diagnóstico. Coma: etiology, pathophysiology and diagnosis. An Pediatr Cont. 2008; 6: 191-202.
7. Simpson D, Reilly P. Pediatric coma scale. Lancet. 1982; 2: 450.
8. Reilly PL, Simpson DA, Sprod R, Thomas L. Assessing the conscious level in infants and young children: a pediatric version of the Glasgow Coma Scale. Childs Nerv Syst. 1988; 4: 30-3.
9. Michelson D, Thompson L, Williams E. Evaluation of stupor and coma in children. Walthman (MA): UpToDate; 2023. Available at: https://www.uptodate.com/.
10.*** Freedman DA, Roach ES. Status Epilepticus. Pediatr Rev. 2023; 44: 383-92.
11. Soto-Insuga V, González-Alguacil E, García-Peñas JJ. Estado epiléptico pediátrico. Pediatric status epilepticus. Rev Neurol. 2022; 75: 225-38.
12. Fernández Carrión F, Fernández de Miguel S. Estatus epiléptico en UCIP. Status epilepticus in PICU. Protoc diagn ter pediatr. 2021; 1: 885-904.
13. Hirsch LJ, Gaspard N, van Baalen A, Nabbout R, Demeret S, Loddenkemper T, et al. Proposed consensus definitions for new-onset refractory status epilepticus (NORSE), febrile infection-related epilepsy syndrome (FIRES), and related conditions. Epilepsy. 2018; 59: 739-44.
14. Blanco Lago R, Huete Hernani B, Ibáñez Micó S. Estatus epiléptico. Status epilepticus. Protoc diagn ter pediatr. 2022; 1: 429-39.
15. Singh A, Stredny CM, Loddenkemper T. Pharmacotherapy for pediatric convulsive status epilepticus. CNS Drugs. 2020; 34: 47-63.
16. McKenzie KC, Hahn CD, Friedman JN. Emergency management of the pediatric patient with convulsive status epilepticus. Paediatr Child Health. 2021; 26: 50-66.
17.*** De Castro de Castro P, Simón de las Heras R. Ictus pediátrico. Pediatric stroke. Protoc diagn ter pediatr 2022; 1: 159-67.
18. Bhate S, Ganesan V. A practical approach to acute hemiparesis in children. Dev Med Child Neurol. 2015; 57: 689-97.
19. Ladner TR, Mahdi J, Gindville MC, Gordon A, Harris ZL, Crossman K, et al. Pediatric acute stroke protocol activation in a children’s hospital emergency department. Stroke. 2015; 46: 2328-31.
20. Phelps K, Silos C, De La Torre S, Moreno A, Lapus R, Sanghani N, et al. Establishing a pediatric acute stroke protocol: experience of a new pediatric stroke program and predictors of acute stroke. Front Neurol. 2023; 14: 1194990.
21. Felling RJ, Rafay MF, Bernard TJ, Carpenter JL, Dlamini N, Hassanein SMA, et al. Predicting recovery and outcome after pediatric stroke: results from the international pediatric stroke study. Ann Neurol. 2020; 87: 840-52.
22. Yaradilmiş RM, Güngör A, Bodur İ, Güneylioğlu MM, Öztürk B, Göktuğ A, et al. Evaluation of Acute Ataxia in the Pediatric Emergency Department: Etiologies and Red Flags. Pediatr Neurol. 2023; 139: 1-6.
23.*** Radmard S, Zesiewicz TA, Kuo SH. Evaluation of Cerebellar Ataxic Patients. Neurol Clin. 2023; 41: 21-44.
24. Segal E, Schif A, Kasis I, Ravid S. Acute ataxia in children: Common causes and yield of diagnostic work-up in the era of varicella vaccination. J Clin Neurosci. 2019; 68: 146-50.
25. Petley E, Prasad M, Ojha S, Whitehouse WP. Investigating ataxia in childhood. Arch Dis Child Educ Pract Ed. 2020; 105: 214-21.
26. Desai J, Mitchell WG. Acute cerebellar ataxia, acute cerebellitis, and opsoclonus-myoclonus syndrome. J Child Neurol. 2012; 27: 1482-8.
27. Wakerley BR, Uncini A, Yuki N; GBS Classification Group; GBS Classification Group. Guillain-Barré and Miller Fisher syndromes-new diagnostic classification [published correction appears in Nat Rev Neurol. 2014; 10: 612]. Nat Rev Neurol. 2014; 10: 537-44.
28. Bodensteiner JB. The evaluation of the hypotonic infant. Semin Pediatr Neurol. 2008; 15: 10-20.
29.*** Mercuri E, Pera MC, Brogna C. Neonatal hypotonia and neuromuscular conditions. Handb Clin Neurol. 2019; 162: 435-48.
30. Jiménez E, García-Cazorla A, Colomer J, Nascimento A, Iriondo M, Campistol J. Hipotonía en el periodo neonatal: 12 años de experiencia. Hypotonia in the neonatal period: 12 years of experience. Rev Neurol. 2013; 56: 72-8.
31. Bustos BR, Díaz F, Cores C, Castro ZF, Cruces P. Mielitis flácida aguda e infección por enterovirus: una enfermedad grave emergente. Acute flaccid myelitis and enterovirus infection: a serious emerging disease. Andes Pediatr. 2022; 93: 552-60.
32. Lupu VV, Miron I, Cianga AL, Gavrilovici C, Grigore I, David AG, et al. Diagnostic Pitfalls in Guillain-Barré Syndrome: Case Report and Literature Review. Children (Basel). 2022; 9: 1969.
33. Goldberg B, Danino D, Levinsky Y, Levy I, Straussberg R, Dabaja-Younis H, et al. Infant Botulism, Israel, 2007-2021. Emerg Infect Dis. 2023; 29: 235-41.
34. Antonucci L, Locci C, Schettini L, Clemente MG, Antonucci R. Infant botulism: an underestimated threat. In Infectious Diseases. 2021; 53: 647-60.
Recommended bibliography
– Freedman DA, Roach ES. Status Epilepticus. Pediatr Rev. 2023; 44: 383-92.
This article provides a complete and updated review of pediatric status epilepticus. It highlights the importance of the pediatrician in the early recognition and treatment of status epilepticus, thus preventing acute and chronic damage that can be associated with status epilepticus.
– De Castro de Castro P, Simón de las Heras R. Ictus pediátrico. Pediatric stroke. Protoc diagn ter pediatr. 2022; 1: 159-67.
Excellent and accessible review of pediatric stroke in our field of work. We recommend reading the Diagnostic and Therapeutic Protocols of Pediatric Neurology of the AEPED. Available at: https://www.aeped.es/documentos/protocolos-diagnosticos-y-terapeuticos-neurologia-pediatrica.
– Radmard S, Zesiewicz TA, Kuo SH. Evaluation of Cerebellar Ataxic Patients. Neurol Clin. 2023; 41: 21-44.
In-depth review of cerebellar ataxias, not only its motor manifestations.
– Mercuri E, Pera MC, Brogna C. Neonatal hypotonia and neuromuscular conditions. Handb Clin Neurol. 2019; 162: 435-48.
Diagnostic approach to neonatal neuromuscular pathology, whose approach scheme is easy to understand and suitable for all audiences.
| Clinical case |
|
A 21-day-old neonate who attends the Emergency Room due to irritability, weakness, and refusal of feedings, during the last 24 hours. No bowel movement in the last 48 hours. Fever, no respiratory symptoms. Family background: healthy non-consanguineous parents. He is the only child of the couple. Personal history: spontaneous pregnancy of normal course. Eutocic delivery at 41 +3 weeks of gestation. Apgar 9/10. Non incidental perinatal period. Normal birth biometry. Currently breastfeeding with good suction and swallowing. Normal metabolic and hearing screenings. Examination: Pediatric evaluation triangle (PET): decompensated shock. Bad general condition. Poor distal perfusion. Eupneic, no respiratory distress. Glasgow Coma Scale 8 (Ocular1, Verbal2, Motor5). The following stands out: whining when crying, absence of spontaneous eye opening, non-reactive bilateral mydriasis, poor spontaneous mobility, global hypotonia and abolished deep tendon reflexes. He was admitted in the Neonatal Unit.
|


