 Behavior disorders
Behavior disorders  |
| Topics on Continuous Training |
A. Díez Suárez*, C. Canga Espina**
*Head of the Child and Adolescent Psychiatry Unit. **Resident of Child and Adolescent Psychiatry. Department of Psychiatry and Medical Psychology, Clínica Universidad de Navarra. Pamplona, Navarra
| Abstract
There are two main behavioral disorders, oppositional defiant disorder (ODD) and conduct disorder. These disorders are usually associated with a wide range of mental disorders or stressful life events. Conduct disorder is usually preceded by oppositional defiant disorder, and symptoms are more severe, being a more advanced complication of ODD. Behavioral disorders may be associated with other psychiatric disorders, mainly Attention Deficit Hyperactivity Disorder, but also with anxiety or depression. The characteristics of each case should be assessed, and an accurate diagnosis should be made in order to propose an adequate therapeutic approach. Both, DSM-5 and ICD-10 offer their own diagnostic criteria. The diagnosis is clinical, through an interview with the patient and his family. Cognitive-behavioral or behavioral psychotherapy is the first-line treatment. Parents or main caregivers must be involved in the therapy. Likewise, the underlying psychopathology must be specifically treated, with medication or specific psychotherapy, if needed. Atypical antipsychotics may be useful for the most severe cases, but they are not recommended as the first choice. |
| Resumen
Los dos principales trastornos del comportamiento son: el trastorno negativista-desafiante y el trastorno de conducta. Por lo general, estos trastornos son secundarios a otras enfermedades o situaciones de índole muy variada. El trastorno de conducta suele venir precedido de un trastorno negativista desafiante, sus síntomas son más graves y, en muchos casos, es una complicación del anterior. En muchos casos, se asocian a otro trastorno psiquiátrico, principalmente al trastorno de déficit de atención e hiperactividad, pero también a ansiedad o depresión. Es muy importante investigar en profundidad las características de cada caso y realizar un diagnóstico preciso, para que el enfoque terapéutico sea correcto. Tanto el DSM-5 como la CIE-10, ofrecen sus propios criterios diagnósticos. El diagnóstico es clínico, mediante una entrevista al paciente y a sus familiares. El tratamiento principal es la psicoterapia, de tipo cognitivo-conductual o conductual, y con la colaboración de los padres o cuidadores principales. Asimismo, se debe tratar de forma específica la psicopatología subyacente, si es preciso con medicación. Algunos fármacos como los antipsicóticos atípicos, pueden resultar útiles para los casos más graves, pero no se recomiendan como primera elección. |
Key words: Behavior disorders; Oppositional-defiant disorder; Conduct disorder.
Palabras clave: Trastornos de comportamiento; Trastorno negativista-desafiante; Trastorno de conducta.
Pediatr Integral 2022; XXVI (2): 68 – 75
OBJECTIVES
- To understand the characteristics of the main behavioral disorders: oppositional-defiant disorder and conduct disorder.
- To know their prevalence and populations in which it appears most frequently.
- To recognize the main risk factors related to behavioral disorders.
- To identify the diverse useful tools to make a correct diagnosis.
- To learn about the different types of effective treatments in behavioral disorders, both psychological and pharmacological.
|
|
|


Behavior disorders
Introduction
If parents consult in clinic because their child “misbehaves”, the pediatrician must inquire about the reasons for him behaving like that, so as to find the best solution.
When a child or adolescent “misbehaves”, that is, he argues or does not follow the rules, it is very important to know his reasons; why he behaves that way. This situation is known in psychiatry and psychology as oppositional defiant disorder (ODD). If, in addition, his behavior becomes more aggressive and the violations of the rules are more severe or with a tendency to disregard the feelings of others, it is labelled as conduct disorder (CD). It is important to be precise with the terms, since the term “conduct disorder” is often used in a loose way to refer to any type of resistance to the norms, when conduct disorders have a specific definition in the main classification systems.
The situations that hide behind behavioral disorders can be of various kinds, and they could be compared to the tip of an iceberg (Fig. 1).

Figure 1. Factors associated with behavioral disorders: Oppositional Defiant Disorder (ODD) and Conduct Disorder (CD) often “hide” other psychiatric disorders or situations that generate stress for the child or adolescent, like the tip of the iceberg.
When parents consult the pediatrician for behavioral anomalies, as professionals we should not be satisfied with a single diagnosis of ODD, this situation would be equivalent to concluding that a child who comes to the clinic with “fever” has “fever”. That is, we have to inquire about the reasons behind the child behaving that way. Adolescence itself is often associated with confrontation of norms, in a desire to reaffirm their own identity, as adolescents move from the stage of childhood to adult life. In some cases, an intense adolescence can manifest as ODD, mainly when the educational pattern is rigid, authoritarian or inflexible. Children’s temperaments can be very different, and some children are more intense in the way they express themselves and behave. Even any adverse situation in the life of a child or adolescent can manifest with these types of symptoms. It can be associated with social situations (psychosocial adversity, lack of adequate supervision and care, bullying of any kind) or family situations (sibling rivalry, parental separation, psychiatric or other illnesses, or death of parents or other family members). In other cases, it responds to the intake of substances of abuse (alcohol, cannabis, etc.). In addition to these factors of a more psychosocial nature, the pediatrician must rule out that this oppositional behavior is associated with other psychiatric disorders, such as Attention Deficit Hyperactivity Disorder, anxiety or depression.
Epidemiology of behavioral disorders
Oppositional defiant disorder is milder than conduct disorder and often precedes it. They appear more frequently in males, with an approximate prevalence of 2-10%.
Conduct disorders are less frequent than oppositional defiant disorder, and as previously mentioned, ODD usually precedes CD. ODD is a frequent reason for consultation in Pediatrics, with a variable estimated prevalence, although most studies place it around 2-10%. These data differ according to data collection criteria, the population studied and the possible cultural differences regarding what is socially accepted(1,2). Both disorders appear more frequently in males than in prepubertal females, between two and three times more, with a tendency to become equal in adolescence(2).
Concept and symptoms of behavioral disorders
Behavioral alterations are frequent and common at different stages of children’s development, especially at 18-24 months of age, with a peak of maximum intensity at 3 years of age, and in adolescence. These behaviors are considered pathological or become part of a disorder category, when they extend far beyond these conditions, both in frequency and intensity.
Both disorders, ODD and CD, are different, have their own diagnostic criteria, and should not be confused. Most children with ODD will not develop symptoms compatible with CT; although retrospectively, it is most likely that patients with CT have met ODD criteria at some point in the past(3). The characteristics of both disorders are summarized below:
• Oppositional defiant disorder:
– It is a generic symptom, a manifestation of unspecific discomfort in childhood.
– Its clinical manifestations vary depending on the context and evolve with age.
– It is characterized by a persistent pattern of anger, irritability, and defiance or vindictiveness that lasts for at least six months and manifests in various settings.
– In general, children have little awareness of disease, that is, they do not usually identify or understand the importance of their manifestations.
• Conduct disorder:
– Age of onset later than ODD, around 14 years-old(3).
– The behavior involves a series of aggressive behaviors towards people or animals, destruction of objects, presence of ruse or theft, and severe violations of the rules.
– It usually leads to legal problems.
– It is usually accompanied by an apparent emotional coldness, which is due to difficulties in putting oneself in another’s place. Several studies associate this behavior with neurobiological abnormalities in some regions, such as the corpus callosum.
Diagnosis of behavioral disorders
Diagnosis of behavioral disorders is clinical, based on an interview with the child and his parents.
As in all psychiatric disorders, the diagnosis of behavioral disorders is clinical, based on interviews with both the patient and his family, primary caregivers and, if necessary, teachers. We must also bear in mind that the clinical manifestations of ODD vary depending on the context and evolve with age. To do this, information must be collected from various sources, in addition to the patient’s own account. Observing the child’s behavior in the interview and his interaction with his parents: how they sit, how they talk to each other, how they look at each other, etc., can be very illustrative of what the situation is like at home. In general, children tend to underestimate this type of difficulties called “externalizing behaviors”; namely, the child with ODD may have little awareness of the problem. However, outside observers provide more details and are often more concerned. This is called informant divergence.
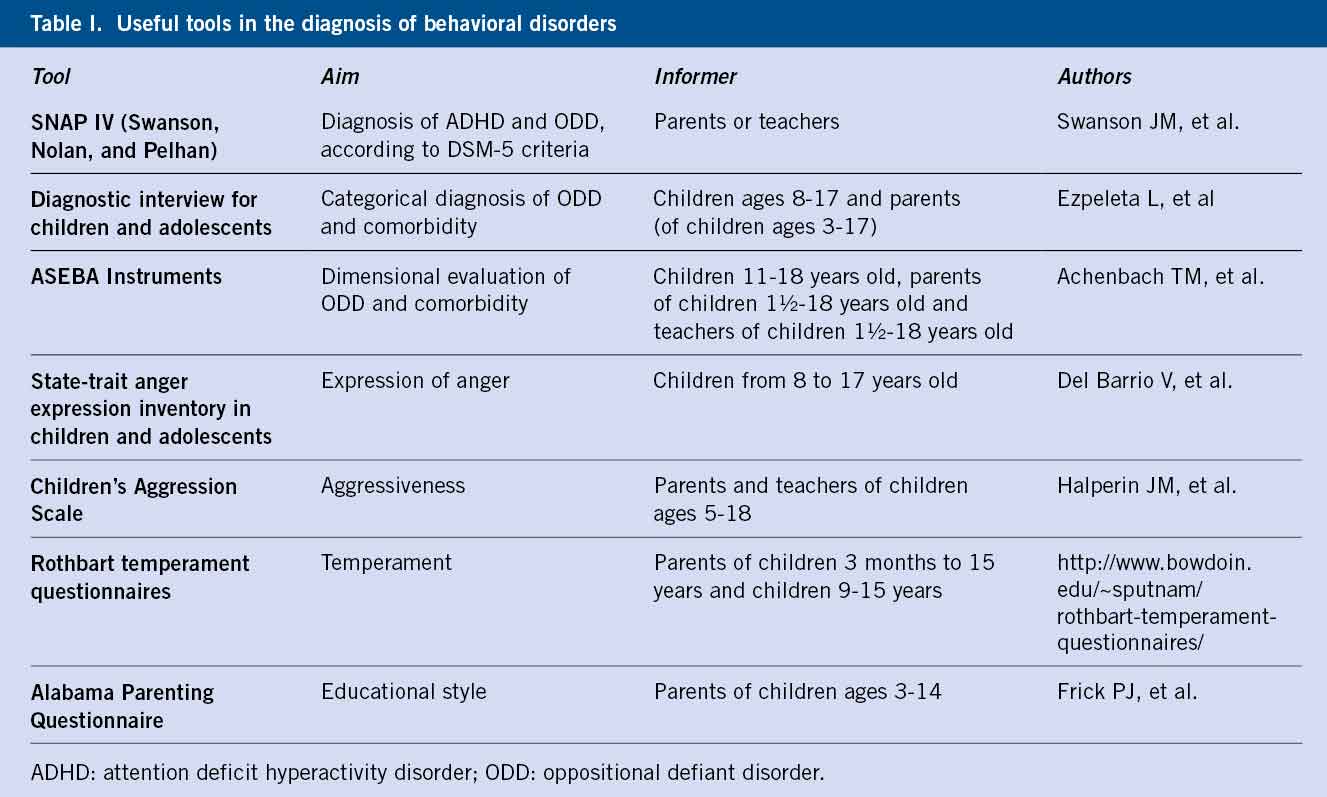
In addition to the clinical interview, some questionnaires can be used, both self- and face-to-face-administered, and structured interviews to detect other symptoms, quantify or grade symptoms, or improve communication in uncooperative children. Table I offers a list of interviews and questionnaires, all of them available in Spanish.
Diagnostic criteria according to ICD10 and DSM-5 (Table II)

ODD and CD can be considered two pathologies within the same spectrum (ICD-10) or two different pathologies (according to DSM-5, ODD precedes CD). DSM-5 classifies ADHD within the “neurodevelopmental disorders” and separates it from the “disruptive, impulse control and behavior disorders”, which include oppositional defiant disorder (ODD), conduct disorder (dissocial) (CD) and impulse control disorders (kleptomania, pyromania and antisocial personality disorder).
Both ICD-10 and DSM-5 criteria for conduct or dissocial disorder require for the symptoms to be present for at least 6 months. 15 behaviors are listed that should be considered for the diagnosis of a conduct disorder, and at least three of them must be present. It should be indicated if the age of onset is before or after 10 years-old. Three subtypes are specified: conduct disorder limited to the family (F91.0), conduct disorder in unsocialized children (F91.1, where the child or adolescent has no friends and is rejected by his peers), and behavior disorder in socialized children (F91.2, where relationships with peers are within normal limits). Behaviors are grouped into four categories:
• Aggression to people and animals:
– He frequently lies and breaks promises in order to obtain benefits and favors, or to avoid obligations.
– He frequently starts physical fights (not including fights with siblings).
– He has used a weapon that could cause serious bodily harm to others (eg, bricks, broken bottles, knifes, firearm).
– He often stays out of the household at night, despite parental prohibition (beginning before age 13).
– Physical cruelty towards other people (eg, tying up, cutting, or burning their victims).
– Physical cruelty to animals.
• Destruction of private property:
– Deliberate destruction of another person’s property (different to setting a fire).
– Deliberately starting a fire with the intention of causing serious damage.
• Ruse and theft:
– Thefts of objects of significant value without confronting the victim, either at home or outside of it (eg: shops, foreign houses, counterfeits).
• Serious breach of the rules:
– Repeated absences from school, beginning before the age of 13.
– Leaving the home at least on two, or on one occasion for more than one night (unless it is to prevent physical or sexual abuse).
– Any episode of violent crime or incident that involves confrontation with the victim (including: “pulls”, robberies and extortion).
– Forcing another person to have sex.
– Frequent bullying of others (eg, deliberate infliction of pain or harm, including intimidation, indecent abuse, or torture).
– Breaking into the home or vehicle of others.
Differential diagnosis
The differential diagnosis must be considered with different pathologies, mainly psychiatric, which can generate symptoms similar to those previously described(7).
Among the psychopathological problems, the following can be found: ADHD, depressive disorders (often, adolescents with depression are more irritable than sad), anxiety disorders, substance abuse disorder, others less frequent (post-traumatic stress disorder, somatization, non-behavioral addictions…). Some diseases or situations can be associated with irritability or oppositional behavior. They are rare in children and adolescents, but the pediatrician should consider them in some specific cases. Most refer to neurological disorders (cranioencephalic trauma, cerebrovascular accidents, confusional syndromes, infections or brain tumors). Metabolic disorders or the effect of certain drugs, such as: corticosteroids, some antiepileptic drugs (perampanel) or others with a stimulant effect (anti-flu), can be confused with an ODD.
Risk factors
In behavioral disorders it is preferable to speak of risk factors than of etiology or causes, as such. As in all psychiatric disorders, there is no single factor that causes behavioral difficulties on its own. Whilst reading this, many pediatricians will share the impression that there are cases of children or adolescents with appropriate behaviors who come from complex environments, broken families, with drug use, physical abuse or neglect. In other cases, despite having “everything in their favor” (parents with an assertive educational style, schools where teachers care about them, lack of exposure to risky situations, drug use, etc.), some adolescents behave in a very defiant way or even develop serious behavior disorders. Broadly speaking, risk factors can be classified into(6): genetic, personal, social and family factors.
Genetic factors
It is estimated that the heritability (percentage of the etiology that can be attributed to genetics) of ODD is around 50%. It is a multigenic inheritance.
In addition to heredity as such, there is a very important interaction between genetics and the environment. In other words, there is the possibility that a child or adolescent with several family members with behavioral problems may not develop it if growing up in a protective environment and vice versa; some boys without that genetic load, but with unfavorable environments can develop ODD or TC. For example, the different functional polymorphisms of the gene promoter of the enzyme monoamine oxidase (MAO) influence the expression of dysfunctional behavior in the presence of child abuse, so that child victims of abuse with a genotype that generates low levels of activity of MAO, develop antisocial behaviors more frequently.
In adoption studies, it has been observed that children with a high genetic risk of behavioral problems receive less assertive parenting from their adoptive parents compared to children with a low genetic risk of behavioral disorders(7).
Personal factors
Male sex is a risk factor for both behavioral disorders, which are between 4 and 5 times more frequent than in females. There is evidence that children who are impulsive, irritable or have marked reactions to negative stimuli (frequent and intense tantrums) from early childhood, are more likely to be defiant throughout the different stages of life(8).
Some children and adolescents with behavior problems easily regret their actions, however, others seem to be unaware of the damage they cause. The so-called antisocial traits, that is, the tendency to act in an insensitive or unemotional way, without considering the feelings of others, are highly heritable and have a neurobiological origin. When they appear, they are associated with greater severity in behavioral disorders.
Poor verbal skills can contribute to behavioral problems, especially at an early age. Children who try to express themselves and do not succeed, or feel that they are not understood, have a greater tendency to act aggressively and disproportionately angry(9).
Social factors
Children with challenging symptoms tend to experience rejection and are often grouped with peers also with problem behaviors. In turn, the fact of frequenting companies of this sort perpetuates these behavioral problems.
It is well known that in the most deprived social classes there are more children with difficulties in regulating their behavior. There are several factors that are associated when talking about low socioeconomic status: the level of supervision by parents, the economic level, access to prevention and care resources are lower, there is more violence in their environment or they are less likely to engage in healthy leisure and free time activities (sports, outdoor activities, art, etc.). Likewise, if they present academic or psychological difficulties, the chances of receiving support are lower than those of more affluent classes(6).
Family factors
The relationship between educational style and children’s behavior is bidirectional: inappropriate parenting styles can worsen, in vulnerable children, oppositional behaviors and, in turn, these challenging behaviors cause greater stress, despair and worsening in parents´ educational strategies. In general, educational lifestyles based on excessive punishment, constant criticism, excessive overprotection or ambivalence aggravate behavioral problems(10). When parents do not provide clear orders or there are disagreements between them, it is more likely that the child will not follow those rules or limits. If the rules are non-existent or very lax, the child himself establishes his rules. If they are criticized for everything they do, children’s chances of changing their behavior are slim. As it will be explained later in the treatment section, undesirable behaviors that receive attention tend to perpetuate themselves, and the consequences of these behaviors must be logical and proportionate. In general, although, of course, not in all cases, in unstructured, single-parent families or if there is psychopathology (especially maternal depression) or drug abuse in the parents, it is easier for the environment to be a facilitator of these behaviors(3).
There is no single condition that causes a behavioral disorder. There are risk factors: genetic, social, family or personal, that can influence its development.
Treatment of behavioral disorders
Psychological and psychosocial treatment
Parental training in behavior modification techniques is essential in all cases of behavioral disorders. When it comes to a mild ODD, with impact limited to the family environment, it is very common for behavioral problems to be resolved only with this type of intervention.
These programs follow a manual and all those professionals in the health or educational field can apply them with the appropriate training: nurses, pediatricians, primary care doctors or psychiatrists, psychologists, educational psychologists, teachers or occupational therapists. In general, they apply to parents or primary caregivers, because they are the ones who spend the most time with the children and, in most cases, are the ones who make the request for help. On certain occasions, it may also be necessary to involve the school, for instance, when the behavioral difficulties are predominantly manifested in the school setting or if they are severe.
There are multiple manualized behavior modification programs, for example:
• “The Incredible Years” from Webster-Stratton (https://incredibleyears.com/team-view/carolyn-webster-stratton/).
• “Triple P” program of positive parenting (https://www.triplep.net/glo-es/home/).
The main objectives of these trainings are: to encourage positive behaviors, to ignore, when possible, negative behaviors, and to establish stable and predictable norms and routines. Parents are taught to praise their children, techniques to ignore such as the use of “time out”, to increase structure and order, to establish clear, simple and concrete rules, to use, on occasion, point systems, to agree immediate consequences in advance (positive if they are fulfilled and negative if they are not fulfilled), propose realistic goals, etc. Table III offers some practical advice for parents.

It is also important to learn to detect the situations that can trigger disproportionate explosions of aggressiveness in the adolescent, in order to try to avoid them. It is especially important to prioritize the demands or “choose the battles”, so that three types of situations are established:
1. Those that are neither important nor dangerous (tidying up the room, finishing dinner, wearing a particular type of clothing or hair), but they generate a lot of explosiveness in children or adolescents if we try to impose our criteria.
• In these cases, it is preferable to let them “get away with it”. It is not worth to intensely argue about this, when there are other more relevant problems pending to be solved.
2. The important and potentially dangerous ones in case he disobeys, such as crossing the street without looking, using drugs or attacking with sharp objects.
• In these cases, parents must enforce their rule, even if it causes an explosion.
3. Those that are neither important nor dangerous, but that are not minor either, such as: the time to arrive home or the type of sport he can choose.
• Parents are encouraged to negotiate with their child until solutions are found that satisfy everyone.
This training with parents is usually effective, because it reduces explosiveness and violent situations, since parents do not have to control everything, but only part of the behaviors. For more information, check this document: http://www.livesinthebalance.org/sites/default/files/SPANISH-PAPERWORK.pdf.
The coordination of the pediatrician with schools, teachers and school counselors is essential when establishing a coordinated plan of action. Likewise, the pediatrician can exchange information and re-establish contact with other professionals involved, such as educators, social service personnel or, if necessary, judicial personnel. In cases of serious behavioral disorders, when families are unable to deal with the situation or if the behavior of the child or adolescent poses a danger to others, it may be necessary to transfer the child to a therapeutic center specialized in behavioral problems. These admissions are considered temporary, and during them an intensive and multidisciplinary approach is carried out with the child and his family.
The treatment of choice is cognitive-behavioral psychotherapy, based on behavior modification strategies, involving the child and his parents.
Pharmacotherapy
Specific to the underlying disorder if present
As explained in the previous sections, it is very common for ODD or CD to be associated with other psychiatric disorders. If the patient has ADHD, he should be treated with stimulants (methylphenidate, lisdexamfetamine) or non-stimulants (atomoxetine, guanfacine). Both groups of drugs have shown their effectiveness in reducing both the core symptoms of ADHD and improving behavior.
If the patient presents depressive or anxiety symptoms, it should be considered whether he is a candidate for specific cognitive-behavioral psychotherapy or whether he needs to add selective serotonin reuptake inhibitor (SSRI) antidepressants. In general, psychotherapy is indicated in cases of mild or moderate intensity, provided that the patient is cooperative, the family can accompany him and if there are trained and experienced professionals. In recent years, online therapy has become an alternative to consider in some situations. When the symptoms are more severe (eg, if anxiety is associated with significant somatizations, sleep is severely affected, or if thoughts of suicide are present), treatment with SSRIs should be indicated, such as: fluoxetine, sertraline, or escitalopram. The use of benzodiazepines should be reserved for specific symptoms and for a limited time.
No drug has shown effectiveness in reducing the consumption of toxic substances, which should be addressed with cognitive-behavioral psychotherapy, with an approach based on acceptance and commitment therapy. In these cases, social measures aimed at limiting access to alcohol and drugs by offering healthy leisure alternatives are very important.
Use of psychoactive drugs for severe behavioral disorders
In some cases, from the beginning, the behaviors presented by the patient entail a high degree of aggressiveness, and can place the physical integrity of the cohabitants at risk. In other cases, initially, the application of psychotherapy may be effective, but over time the situation worsens. In any of these situations, adding atypical antipsychotics (risperidone, aripiprazole, olanzapine or quetiapine) can be considered. This is applicable for both TND and TC. They should be used in the lowest possible doses and for a specific period of time, due to their potential adverse effects. Whenever the prescription of this type of drug is considered, the pediatrician must ensure that other perpetuating factors that may be treatable have been reviewed in detail(11).
These drugs help reduce aggressiveness and irritability, making it more likely that the management that adults perform at home and in the school is effective and that parents can better work with what they have learned in the sessions of behavioral therapy with the psychologist.
Pharmacological treatment for behavioral disorders should be indicated if there is any other underlying psychiatric disorder. Antipsychotics are not a treatment of first choice.
Role of the Primary Care pediatrician
Some of the roles of the Primary Care pediatrician in behavioral disorders (ODD and TC) are:
• To identify the main risk factors that can be associated with behavioral disorders.
• To recognize the symptoms of ODD and TC, as well as the underlying situations to which they can be associated, so as to establish an early adequate diagnosis.
• To establish an adequate communication, both with the family and with other professionals involved: teachers, school counselors, educators, social and judicial services.
• To apply or indicate behavior modification programs aimed at parents or the children themselves.
• To indicate pharmacological treatments in cases in which another psychiatric disorder is identified, such as ADHD, depression or anxiety.
Conflict of interest
There is no conflict of interest in the preparation of the manuscript. Declaration of interests: none.
Bibliography
1. Rodríguez Hernández PJ. Trastornos del comportamiento. Pediatr integral. 2017; XXI: 73-81.
2. Ogundele MO. Behavioural and emotional disorders in childhood: A brief overview for paediatricians. World J Clin Pediatr. 2018; 7: 9-26.
3. Rowe R, Maughan B, Pickles A, Costello EJ, Angold A. The relationship between DSM-IV oppositional defiant disorder and conduct disorder: findings from the Great Smoky Mountains Study. J Child Psychol Psychiatry. 2002; 43: 365-73.
4. ICD-10. Mental and Behavioral Disorders. Tenth Revision of the International Classification of Diseases. Clinical descriptions and diagnostic guidelines. World Health Organization, Geneva. 1992.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. 2013.
6. Azeredo A, Moreira D, Barbosa F. ADHD, CD, and ODD: Systematic review of genetic and environmental risk factors. Res Dev Disabil. 2018; 82: 10-9.
7. Ouellet-Morin I, Côté SM, Vitaro F, Hébert M, Carbonneau R, Lacourse É, et al. Effects of the MAOA gene and levels of exposure to violence on antisocial outcomes. Br J Psychiatry. 2016; 208: 42-8. doi: 10.1192/bjp.bp.114.162081. Epub 2015 Oct 22. PMID: 26494873.
8. Stringaris A, Maughan B, Goodman R. What’s in a disruptive disorder? Temperamental antecedents of oppositional defiant disorder: findings from the Avon longitudinal study. J Am Acad Child Adolesc Psychiatry. 2010; 49: 474-83.
9. Smith AK, Stasi SM, Rhee SH, Corley RP, Young SE, Hewitt JK. The Role of Attention-Deficit/hyperactivity Disorder in the Association between Verbal Ability and Conduct Disorder. Front Psychiatry. 2011; 2: 3.
10. Fooladvand M, Nadi MA, Abedi A, Sajjadian I. Parenting styles for children with oppositional defiant disorder: Scope review. J Educ Health Promot. 2021; 10: 21.
11. Loy JH, Merry SN, Hetrick SE, Stasiak K. Atypical antipsychotics for disruptive behaviour disorders in children and youths. Cochrane Database Syst Rev. 2017; 8: CD008559.
Recommended bibliography
– Quy K, Stringaris A. Oppositional defiant disorder. Irarrázaval M, Andres Martín (eds.) Prieto-Tagle F, Gilibert Sánchez N (trans.). In Rey JM (ed.), IACAPAP Child and Adolescent Mental Health Manual. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions 2017. Available at: https://iacapap.org/content/uploads/D.2-Oppositional-Defiant-Dis-Spanish-2017.pdf.
This chapter summarizes, in a highly up-to-date manner, the main evidence on the etiopathogenesis and therapeutic approach of ODD. It can be found online free of charge in the link provided and translated into several languages.
– Scott S. Conduct Disorder (Irarrázaval M, Martín A, eds.; Prieto Tagle F, Hacohen Domené S, trans.). In King JM (ed.). IACAPAP Child and Adolescent Mental Health Manual. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions 2017. Available at: https://iacapap.org/content/uploads/D.3-Conduct-Disorder-Spanish-17.pdf.
This IACAPAP updated review article, which is available for free online, explains the basics of conduct or dissocial disorders.
– Child mind institute: https://childmind.org/es/guia/guia-rapida-sobre-el-trastorno-de-conducta/.
On this web site clear, concise and very interesting materials for parents and teachers can be found.
| Clinical case |
|
Anamnesis Iker is a 13-year-old teenager who lives at home with his parents and his two older brothers. At the time of the consultation, he has finished the second year of Compulsory Education at the school in his hometown, with acceptable academic performance, although both his parents and teachers consider that he is “below his performance, since he hardly studies”. He attends the consultation accompanied by his parents, due to aggressiveness in the family setting and oppositional behavior at school. For about a year, they have had many conflicts with Iker due to his decline in academic performance, which they attribute to “sloppiness” and this has generated arguments and fights. He fails exams and then passes them in several subjects, he is not organized, he does not write anything down in the school agenda and, he often is unaware of what needs to be studied for the exam. He reports that: “he gets distracted, loses attention and motivation to participate in class, he quickly becomes tired of studying.” Parents describe outbursts of temper, disproportionate to the situation, which have been occurring over the last 6-8 months. They do not identify apparent triggers, apart from “adolescence”. They have been especially concerned in this last month, since on several occasions he has attacked his father with greater force and has threatened to kill him with a knife. On one occasion, he told his mother that he had thought about “burning his father in his sleep”. When inquired about it, he admits that he “thought about it for a short while, whilst his father was pinning him to the ground with his knee on his chest.” The father also admits difficulties in controlling his own impulses, experiences his son’s attitude as a challenge and has repeatedly blamed him for the arguments and bad atmosphere in the family. He has never had fights with friends or other violations of the rules. There is no suspicion of alcohol, tobacco or other drug intake (“it disgusts me”). His use of the Internet and video games is described by his parents as problematic, since if his time was not limited, he would be able to spend “more than 8 hours” watching videos or playing video games of violent content. When they try to negotiate the time spent or when they have the devices removed, he often has angry outbursts. He used to play handball, but gave it up the previous year. Personal history: not relevant. He does not take any medication. Psychiatric family history: none referred Examination and ancillary tests Conscious, oriented in person, space and time. Appropriate behavior and collaborative (calm and approachable at all times). He does not present abnormal movements or psychomotor restlessness. Good performance in memory tasks (working and long-term memory) and abstraction. He presents symptoms of inattention, such as making careless mistakes, being self-absorbed and not seeming to listen to what is being said, avoiding activities that require mental effort and leaving tasks half done, being disorganized and forgetful (loses things), and being easily distracted by external stimuli. He also has some symptoms of hyperactivity and impulsivity, such as being restless, talking excessively, interrupting conversations, or responding impulsively before finishing a question. His speech is fluent, coherent, informative, without alterations of the course or the content. Absence of alterations of sensoperception or the experience of the Self. Dysphoric mood with irritability and some sadness, although he refers “I am no longer with that tension as before”. No anhedonia. Thoughts of uselessness, “I do many things wrong”, and low self-esteem. He does not feel validated by his parents: “my parents want me to be like them, to study and help at home and then to do free work for the community, they don’t love me the way I am”. Parasuicidal gestures. He refers having self-harmed himself through superficial cuts as a way for his parents to be with him. He feels that his parents only scold him and are not with him affectively. He has thought about choking to death, but currently reports that he has no death wishes. He has had several episodes of explosive anger with heteroaggressiveness. He likes fire and burning things. He denies having performed violent acts on animals. He enjoys animated violence, although he is sensitive and suffers when he sees actual violence. No obsessive-compulsive or (hypo)manic symptoms. He is reluctant to go to bed to sleep and has trouble getting up in the morning, but sleeps well. Preserved appetite. He recognizes having difficulties and is open to the possibility of receiving treatment. When requested to formulate three wishes, he asks: 1) “for the reptilian (violent) part of the being to be removed from all humans”; 2) “for atmospheric conditions to improve”; and 3) “having a pill that cures all diseases”. Questionnaires ADHD-RS.es questionnaire (symptoms of inattention and hyperactivity), according to his parents: • Attention deficit: 17 points (abnormal), meets 8/9 criteria. • Hyperactivity: 5 points (normal), meets 0/9 criteria. • Total: 22 points (abnormal).
|
