Acute abdomen
Acute abdomen  |
| Topics on Continuous Training |
R. Hernández Rastrollo, V.P. Silvero Enríquez
Pediatric Service. Pediatric ICU. Badajoz Maternal and Child University Hospital
| Abstract
Acute abdominal pain is a common reason for consultation in pediatric emergencies; Although a low percentage will be due to serious processes, distinguishing them early from the more banal and frequent causes can be a challenge. The age of the child significantly influences the diagnostic possibilities. Carrying out a detailed anamnesis and a meticulous physical examination remain the cornerstones for diagnostic guidance. The judicious use of some complementary tests may be necessary in doubtful cases, among them the usefulness of ultrasound stands out, as it is minimally invasive and provides useful information in many cases. In this review we address, together with the analysis of the large syndromic groups, some of the most frequent causes of acute abdomen in pediatric age. We also point out the importance of good analgesia, provided even before the physical examination, which without hiding the key signs, provides comfort to the child and allows the physical examination to carried out with the necessary tranquility. |
| Resumen
El dolor abdominal de aparición súbita es un motivo frecuente de consulta en Urgencias pediátricas; aunque un bajo porcentaje será debido a procesos graves, distinguirlos precozmente de las causas más banales y frecuentes puede ser un reto. La edad del paciente influye significativamente en las posibilidades diagnósticas. Realizar una detallada anamnesis y una exploración física meticulosa, son los pilares básicos para la orientación diagnóstica. El uso juicioso de algunos exámenes complementarios puede ser necesario en casos dudosos; entre ellos, destaca la utilidad de la ecografía, por ser poco invasiva y proporcionar información útil en muchos casos. En esta revisión abordamos, junto al análisis de los grandes grupos sindrómicos, algunas de las causas más frecuentes de abdomen agudo en la edad pediátrica. Señalamos también la importancia de una buena analgesia, suministrada antes incluso de la exploración, que sin ocultar los signos claves, proporciona confort al niño y permite realizar el examen físico con la tranquilidad necesaria. El dolor abdominal de aparición súbita es un motivo frecuente de consulta en Urgencias pediátricas; aunque un bajo porcentaje será debido a procesos graves, distinguirlos precozmente de las causas más banales y frecuentes puede ser un reto. La edad del paciente influye significativamente en las posibilidades diagnósticas. Realizar una detallada anamnesis y una exploración física meticulosa, son los pilares básicos para la orientación diagnóstica. El uso juicioso de algunos exámenes complementarios puede ser necesario en casos dudosos; entre ellos, destaca la utilidad de la ecografía, por ser poco invasiva y proporcionar información útil en muchos casos. En esta revisión abordamos, junto al análisis de los grandes grupos sindrómicos, algunas de las causas más frecuentes de abdomen agudo en la edad pediátrica. Señalamos también la importancia de una buena analgesia, suministrada antes incluso de la exploración, que sin ocultar los signos claves, proporciona confort al niño y permite realizar el examen físico con la tranquilidad necesaria. |
Key words: Acute abdomen; Appendicitis; Intestinal invagination.
Palabras clave: Abdomen agudo; Apendicitis; Invaginación Intestinal.
Pediatr Integral 2024; XXVIII (1): 17 – 26
OBJECTIVES
• To recognize the main causes of acute abdomen in different age groups.
• To understand the pathogenesis of the various clinical syndromes that may occur, such as acute abdominal pain and its differential diagnosis.
• To acknowledge the need to provide early analgesia.
• To identify the history and examination findings most suggestive of severe acute abdomen.
• To make judicious use of complementary exams and understand their limitations.
• To be familiar with the indications for hospital referral.
|
|
|


Acute abdomen
Introduction
Acute abdominal pain is a very common reason for consultation in pediatric emergency rooms, but most are due to mild and self-limiting processes. Early diagnosis of severe forms, which are time-sensitive, is important, but also avoiding unnecessary invasive tests or treatments.
The proportion of children evaluated in Emergency Departments who present abdominal pain as the main reason for consultation is estimated at 5%, but only between 1% and 8% of them will require hospital admission or surgical examination(1,2). The majority, therefore, are related to medical processes, generally of little severity. However, it is often challenging to differentiate cases of acute abdominal pain that will require urgent surgery from those that will not; and within these, those that are due to mild and more or less self-limited processes, to those that are a consequence of less frequent entities or that require specific treatments.
Understanding the various types and causes of abdominal pain helps identify which patients have a condition that will not improve without medical or surgical intervention. In general, a careful history and a meticulous and repeated physical examination, combined with the judicious and selective use of complementary tests, allow the clinician to differentiate the child who requires urgent action from the one who will benefit from conservative treatment(2-4). Sometimes this decision cannot be made after the initial examination and a period of observation will be necessary. Most cases of acute abdominal pain resolve spontaneously.
Early diagnosis of processes that are time sensitive is important; that is, those whose diagnostic/therapeutic delay may entail a greater risk of complications or increased morbidity, as may occur in the case of appendicitis or intestinal intussusception. On the other hand, it is also desirable not to fall into overdiagnosis, and to perform invasive tests or treatments in patients who do not require it.
Pathophysiology and syndromic conditions
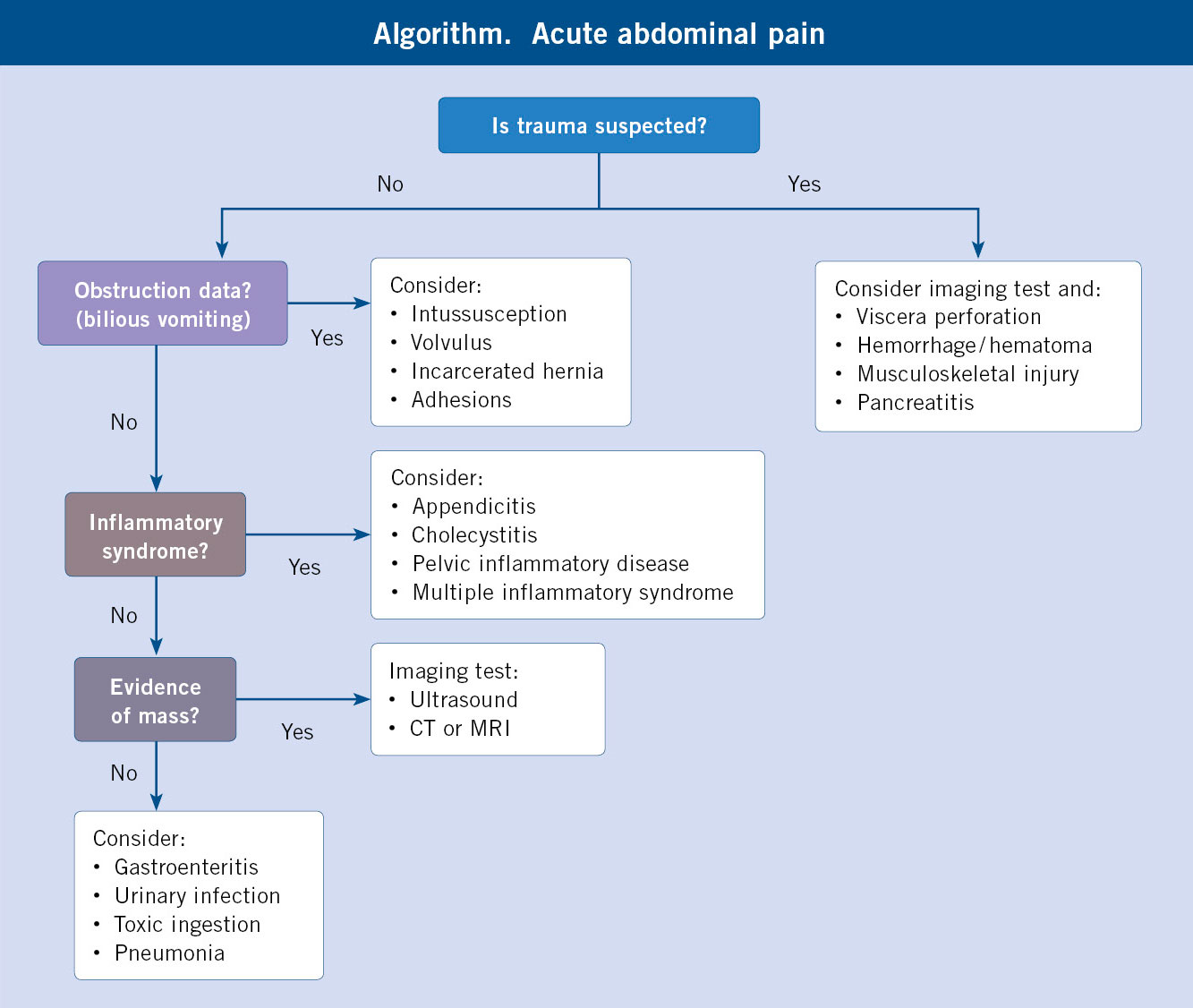
The pain manifests with a diverse symptomatic procession, which helps in the diagnostic approach. Four major syndromes are described: inflammatory, occlusive, traumatic and adnexal.
The sensation of abdominal pain is transmitted to the central nervous system by somatic and visceral afferent fibers. The visceral afferent system innervates the visceral peritoneum and the structures it covers. Visceral pain is poorly localized, but, in general: pain that originates in structures derived from the foregut (stomach, duodenum, pancreas) is located in the epigastrium; pain originating in the midgut (small intestine and colon up to the splenic flexure) is located in the periumbilical region; and pain from hindgut structures is experienced in the hypogastrium. On the contrary, pain originating from the parietal peritoneum (e.g., inflammation) and in the abdominal wall (e.g., muscle trauma) is detected by somatic afferent fibers and is well localized(4,5).
Referred pain occurs as a result of the convergence of visceral and somatic pain pathways in the spinal cord or central nervous system. Pain originating in the abdominal viscera can therefore be perceived as originating in a distant somatic location(4,5). For example, irritation of the diaphragm secondary to pancreatitis, cholecystitis, liver abscess, or splenic hemorrhage may be referred to as pain originating in the lower neck and shoulders, because the diaphragm and shoulder pain pathways converge at the spinothalamic bundles at the level of C4. Similarly, gallbladder inflammation may be experienced in the right infrascapular region, pancreatic pain in the posterior flank, a migrating ureteral stone may be felt as progressing toward the ipsilateral groin, and rectal and gynecologic pain in the sacral area. On the other hand, pain originating in somatic locations, such as the right pleural surface in pneumonia, can be perceived as coming from the lower part of the abdomen, because the afferents from the two regions converge at the level of D10-11. Therefore, it must be taken into account that the location of pain does not always correspond to a problem in said anatomical position(2-5).
Syndromes associated with acute abdominal pain(3-5)
Inflammatory syndrome
The pain is caused by irritation or inflammation of the peritoneum, usually due to an infectious process. In general, it is an intense but localized pain, and it is possible to find an antalgic posture, in which the patient remains still. The patient will avoid walking or will walk slowly and stooped. There may be signs of guarding and decreased peristaltic sounds. When perforation of a hollow viscera has occurred, the symptoms are exacerbated and there is usually abdominal distention and rigidity of the abdominal muscles.
Occlusive syndrome
It occurs when there is a difficulty in normal intestinal transit, whether of mechanical or dynamic origin (paralytic ileus). It is usually accompanied by distention of the intestine proximal to the occlusion, which can translate into clinically evident abdominal distention. It is usually accompanied by vomiting, which could be bilious, and other vegetative symptoms, such as paleness and sweating. The pain is usually poorly located and the patient cannot find an anti-pain posture, which is why they show restlessness. A very similar condition can occur due to obstruction of other digestive or extradigestive ducts with smooth muscles, such as the bile and pancreatic ducts or the ureter.
Trauma syndrome
It appears as a consequence of abdominal trauma that causes peritoneal irritation, usually due to the presence of blood or digestive contents in the peritoneal cavity. Trauma history is not always evident, and may not have been perceived by an adult or may even be hidden (cases of abuse). The majority are closed traumas and the most affected are the solid viscera: spleen and liver.
Adnexal syndrome
It is a consequence of abnormalities in the genital apparatus. In men, the most common causes are testicular torsion, epididymitis, and testicular trauma. In women, physiological processes of puberty predominate: ovulation or dysmenorrhea, but it is necessary to take into account pathologies such as: torsion of ovarian cysts, ectopic pregnancies and pelvic inflammatory disease in sexually active adolescents.
Diagnosis
The diagnosis is based mainly on careful physical examination of the abdomen, after a detailed history.
The keys to the etiological diagnosis of acute abdominal pain are based on: detailed and directed history, methodical abdominal and systemic physical examination and rational use of complementary tests(1,3,5). Age and sex must be taken into account, as they greatly influence the diagnostic possibilities(3-5).
To evaluate the severity of the process, it is useful to initially apply the pediatric evaluation triangle, which may be compromised in more evolved processes, and must be accompanied by checking vital signs: temperature, heart rate, oxyhemoglobin saturation and blood pressure.
Clinical history
As previously mentioned, the age of the child helps to restrict the diagnostic possibilities(2,4) (Table I).

The existence of recent trauma or surgery is also relevant. Other data of potential interest are: foods consumed, medications received, access to toxics or drugs, gynecological or obstetric history, previous episodes similar to the one that motivated the consultation and other previous personal and family pathologies that are considered of interest. In recent years, the history of having suffered from COVID-19 has become especially relevant, due to the high frequency of severe digestive symptoms, sometimes mimicking an acute abdomen, in children with multisystem inflammatory syndrome, weeks after having suffered from COVID-19, symptomatic or not(6,7). Psychosocial history should be considered, as it could contribute to possible somatization.
Although the existence of previous episodes of abdominal pain usually points towards chronic abdominal pain, it cannot be ruled out that these children a priori have an acute abdomen, so it must be examined in each case(2).
Regarding the characteristics of pain, the characteristics of presentation, intensity, type and duration of pain, location and associated symptoms, both digestive and extradigestive must be investigated.
The mode of presentation can be: acute, gradual or intermittent. Sudden onset pain is more likely to be related to cramping, perforation, or acute ischemia (torsions, volvulus). Pain that begins more slowly is more associated with inflammatory processes such as appendicitis, pancreatitis and cholecystitis. Colic is a consequence of spasm in a hollow muscular viscera, usually due to obstructive processes. It is an intense pain, cramping and intermittent in intensity, alternating intervals in which the pain is less intense, although it is still present. During episodes of more intense pain, the patient is restless and often pale and sweaty, without finding a comfortable position. As previously stated, in these cases, problems related to hollow viscera (digestive tube, biliary tree, pancreatic duct, urinary system, uterus and tubes) must be suspected. Inflammatory pain secondary to peritoneal irritation usually results in an immobile, sick-looking patient, in whom the pain is exacerbated by movement(2,4).
Regarding intensity, type and duration, these are subjective data that are not always easy to determine. Scales appropriate to the child’s age can be used to assess intensity. Intense and continuous abdominal pain lasting more than six hours is suggestive of surgical pathology, since it occurs more in relation to acute inflammatory processes; while colicky pain suggests obstruction of the intestinal or genitourinary tract. Intense diffuse pain can occur in situations that evolve from the previous ones(2-5).
Associated symptoms
Fever, lethargy, irritability, anorexia, or paleness may be present. It is unusual for a patient with appendicitis to be hungry. The child with intussusception is lethargic and pale. The presence of symptoms of upper respiratory infection or viral infection may suggest mesenteric adenitis. Dysuria leads to urinary infection. In Schönlein-Henoch vasculitis there is usually a characteristic purpuric rash and periarticular edema, but abdominal pain sometimes appears before these signs.
The presence of other digestive symptoms is common and should be specified. The presence of vomiting, indicating its appearance, for example, whether it is bilious or bloody, is relevant. The frequency and consistency of bowel movements, as well as the presence of blood or mucus in them should be inquired.
The presence of fever, abundant loose stools, and vomiting suggests the diagnosis of gastroenteritis. However, especially in young children, other possibilities that could imitate or seriously complicate this condition must be considered.
Examination
It is necessary to inspect, auscultate and palpate the abdomen. This must be done calmly and after the administration of appropriate analgesia.
Exploratory findings are more important for diagnostic guidance than any complementary test. It is necessary to inspect, auscultate and palpate the abdomen. But for it to be reliable, it is desirable to do it calmly and without haste, after the administration of appropriate analgesia(8).
The examination of the abdomen should be carried out after removing the clothing or diaper, evaluating the presence of distension, old scars, lumps or skin lesions of any type. Also, the abdomen is auscultated to assess the appropriateness of intestinal sounds and, finally, palpation is performed. Achieving calmness in the child during the examination may not be easy, so we must make a careful and thoughtful approach, leaving the presumably most painful region for last. The presence of focal pain or its intensity may be relevant to guide the diagnosis. Palpation also allows detecting involuntary guarding or rebound pain on percussion or decompression suggestive of peritoneal irritation. However, the younger the child, the less reliable the clinical signs of peritoneal irritation are(9). We must also look for hepatomegaly or splenomegaly and locate other possible palpable masses. To palpate the lower border of the liver or spleen, we must start from the inguinal region and ascend towards the subcostal region, since important organomegaly may go unnoticed if the examination begins in the middle part of the abdomen. Next, the inguinal region is examined, looking for the presence of hernias, and the genitals. Examination of the testicles in children with abdominal pain should be carried out with care, since testicular trauma, testicular torsion, and epididymitis may be accompanied by diffuse abdominal discomfort. A swollen and painful testicle with the absence of the cremasteric reflex on the affected side is suggestive of testicular torsion and thus, an urgent ultrasound should be performed.
Anal examination can detect obvious fissures or strictures. A rectal examination can be uncomfortable and should not be done routinely. When considered necessary, it should be performed by the clinician who can best take advantage of the information (e.g., the surgeon, if a surgical pathology is suspected, or the gynecologist, in the case of an adolescent with possible inflammation of the adnexa).
When the diagnosis is doubtful, re-examination of the patient may be necessary, which may be difficult if the initial exam has been painful or stressful, which is why we insist on the need for a careful approach and with prior analgesia.
Complementary exams
The test with the best performance is the abdominal ultrasound. The normality of the complementary exams does not exclude the diagnosis of acute surgical abdomen.
In many of our patients, the diagnosis can be made with the data obtained exclusively from the history and physical examination(2-5). Additional tests should be reserved for cases in which the diagnosis is unclear, or when the test can confirm or rule out significant pathology. It must be kept in mind that early guidance of an acute abdomen is important, which may require time-dependent action, but it is also important to avoid unnecessary tests, especially if they are bothersome or invasive. The diagnostic possibilities are multiple, as previously discussed, and so are the possible tests available in each case. It will be the specific clinical situation that should guide the clinician in the selection of one or more complementary tests.
Imaging techniques
Abdominal ultrasound is a technique with multiple advantages (wide availability, absence of radiation, little discomfort and provides a lot of information), which has made it one of the most used in patients with acute abdominal pain(10,11). It is diagnostic, with considerable certainty, in cases of intestinal intussusception and contributes, in many cases, to the diagnosis of acute appendicitis or another type of inflammatory peritoneal pathology. In addition, it allows visualization of the viscera, so it can be of great help in detecting pathology: pancreatic, renal, hepatic-biliary, splenic or internal genitalia in women. Likewise, it provides us with information about any palpable mass. Doppler technique is of great help in the diagnostic orientation of the acute scrotum. In the case of traumatic acute abdomen, a “bedside” ultrasound, performed by an experienced clinician, provides potentially very useful information for a first assessment of the damage caused.
The indiscriminate routine use of plain abdominal radiography, as a screening tool for abdominal pain, is not recommended due to its low profitability. It is useful in cases of suspected intestinal obstruction, where a standing abdominal X-ray allows the observation of air-fluid levels, and when there is suspicion of pneumoperitoneum or foreign body ingestion. In other types of pathologies, its rational use may have some usefulness to support a doubtful diagnosis, for example: the detection of appendicoliths, antalgic scoliosis or the loss of the psoas shadow would support the diagnosis of appendicitis. The presence of calcifications can put us on the track of urinary stones or even tumor pathology, such as teratomas or neuroblastoma(2,4).
Other imaging techniques, such as computed tomography (CT) or magnetic resonance imaging (MRI), are not routinely used in the initial evaluation of acute abdomen, but may be useful in selected cases(12). CT has the significant disadvantage of the radiation exposure it entails. Its use should be reserved for patients in whom ultrasound has not been decisive and a high degree of suspicion of significant pathology remains. It is considered the most sensitive test for pediatric nephrolithiasis. It can also support the diagnosis of appendicitis in doubtful cases and may be necessary in patients with abdominal trauma, when ultrasound is not sufficiently decisive. MRI has important limitations, such as its long duration and the need for patient sedation. Its performance for the diagnosis of appendicitis is similar to CT.
Biological tests
They provide information, which can be useful, but is rarely decisive in establishing the diagnosis(2,4). The presence of leukocytosis with neutrophilia is common in acute inflammatory pathology, so it would support this diagnostic possibility, without ruling out other options. Equal value would offer the elevation of acute phase reactants, such as C-reactive protein (CRP) or procalcitonin (PCT), although their normality does not allow ruling out the possibility of acute surgical abdomen. Other data from the blood count, such as thrombocytopenia with the presence of schistocytes, would point towards a hemolytic-uremic syndrome, and anemia would indicate sustained blood loss, although it does not allow detection of recent acute bleeding.
In patients with affected general condition or signs of dehydration, urgent blood biochemistry is useful, which allows detecting: hydroelectrolyte abnormalities, alterations in glycemia and renal function. The detection of hyperglycemia could be due to stress, but if it is very high, it could indicate diabetic ketoacidosis, which would be consistent with the finding of ketonemia and the presence of glycosuria. The quantification of liver enzymes and lipase and amylase can guide in cases of hepatobiliary or pancreatic involvement.
A urine analysis (sediment study and culture) should be systematically performed when abdominal pain is accompanied by voiding symptoms. It is also indicated in infants, in whom urinary tract infection is part of the differential diagnosis of abdominal pain. In postmenarchal girls, a pregnancy test and, in both sexes, tests to detect sexually transmitted diseases should be considered.
Main causes of acute abdomen in the pediatric age
Acute appendicitis remains the most common cause of surgical acute abdomen in childhood. The keys to its diagnosis are: history and careful physical examination. In children under 3 years of age, the most common cause of abdominal emergency is intestinal intussusception. In both cases, abdominal ultrasound can be of great help, with greater sensitivity for intussusception than for appendicitis.
Acute appendicitis
It is the most common cause of surgical abdomen in children, diagnosed in up to 8% of patients evaluated in pediatric emergency rooms for acute abdominal pain(13). It has a peak incidence in the second decade of life, especially between 6 and 12 years(5) and, below this age group, its diagnosis represents a challenge due to more non-specific symptoms and a higher rate of complications in its clinical course.
Physiopathologically, an obstruction of the cecal appendix occurs, either by fecal material, lymphoid follicles, fecaliths or appendicoliths, producing, therefore, colicky pain with its distension, which explains why it is poorly focused or predominantly periumbilical. Subsequently, it dilates, with bacterial overgrowth, inflammation, ischemia and, finally, necrosis of the wall, shifting the location of the pain described by the child to the right iliac fossa (RIF). The release of bacteria into the peritoneal cavity will produce initially circumscribed peritonitis, and this will be generalized if the infection is not contained by the intestinal loops and the omentum(14). This sequence allows us to differentiate the 4 evolutionary stages of acute appendicitis (congestive or classically catarrhal, phlegmonous, gangrenous or suppurative, and perforated)(5). The risk of perforation increases with time of evolution, being rare in the first 12 hours of onset of symptoms, and maintains an inverse relationship with the patient’s age, with a rate greater than 50% in children under 5 years of age and among 10-20% in people over 12 years of age(13).
There are some anatomical and physiological characteristics that play a determining role in this clinical course. During the first years of life, the appendix is funnel-shaped, instead of its characteristic vermiform appearance, which makes its obstruction less likely and justifies its lower incidence in this age group. Furthermore, the lymphoid follicles dispersed throughout the colonic epithelium and lining the interior of the appendix reach their maximum size in adolescence. The omentum in preschoolers is thinner and underdeveloped, which hinders its ability to contain the infection, and makes diffuse peritonitis more likely after perforation in this age group(13).
Clinically, they will present: anorexia, initial periumbilical pain that migrates to RIF around 24 hours after onset, with vomiting, which characteristically begins after the onset of abdominal pain(13), and fever that is usually inconstant and low grade, between 24 and 48 hours after the start of the symptoms. When the peritoneum is already involved, either due to irritation or perforation, the abdominal pain is more defined and florid, with other possible accompanying signs (although their absence does not exclude the diagnosis), such as: exacerbation of the pain with cough; when trying to get on the stretcher or asking the child to jump on one leg; involuntary defense with abdominal palpation; pain in the right iliac fossa when exploring the left (Rovsing sign); pain when flexion and internal rotation of the right hip (obturator sign)(14); or pain on extension of the right hip (iliopsoas sign, characteristic of retrocecal appendicitis); in addition to Blumberg’s sign, when pressing the right iliac fossa for a few seconds and suddenly decompressing, triggering intense pain. Children under 5 years of age, on the other hand, present much more diffuse and less localized symptoms, added to the difficulty of verbalizing them(15). A sudden decrease in pain intensity can translate into a perforation as the pressure on the appendiceal wall is reduced(14). Other less frequent symptoms in appendicitis and more related to other processes that are part of its differential diagnosis should not mislead us: diarrhea is frequent in the preschool stage and appears in advanced stages, in which peritonitis also ends up irritating the terminal small intestine and colon; constipation, on the other hand, may appear at the beginning of the clinical picture due to ileus after periappendiceal inflammation; and they can present with urinary symptoms due to bladder irritation and even present leukocyturia or hematuria in a urine test strip (especially in retrocecal cases or in intimate contact with the pelvis)(16).
The cornerstone of diagnosis is a detailed compatible clinical history together with a careful abdominal examination. Classically, the administration of analgesia was avoided prior to the clinical assessment, due to the possibility of masking an abdomen that could require a surgical approach, but current literature has shown that the use of analgesics (even major opioids, if necessary for pain intensity) do not modify the diagnosis of appendicitis or increase the risk of complications due to late screening(5,13).
The analytical study is not usually decisive, as it shares findings with other entities that are part of the differential diagnosis: there is usually a discrete leukocytosis at the expense of neutrophilia and a moderate elevation of CRP occurs. There are studies that are beginning to incorporate other markers such as PCT and calprotectin, with a high negative predictive value, to rule out appendicitis in case of normality, but, today, they are not part of the general diagnostic arsenal(13). Hyponatremia and hyperbilirubinemia have been related to complicated appendicitis(14).
Abdominal ultrasound is the most profitable test, but not mandatory as the combination of clinical and analytical tests is usually sufficient to establish a clinical judgment and indicate mandatory surgical treatment. For its sensitivity and specificity to exceed 90% the appendix must be visualized, and this is the greatest limitation of the technique(17): it is operator-dependent, appendages with abnormal morphologies or dispositions, or the adiposity of the child, which can increasingly represent a greater obstacle, by not offering an optimal examination window. The most suggestive signs are: a diameter greater than 6 mm, non-compressibility, wall thickening greater than 2 mm or the presence of an appendicolith. Other indirect signs, but useful to aid the diagnosis in doubtful cases, are: the rarefaction of the pericecal fat, the presence of free fluid or the unstructured appearance of the appendiceal wall. The abdominal x-ray is increasingly out of use, since irradiation is not justified, there are other less invasive techniques that provide more information. It would only be indicated if there is reasonable doubt of an intestinal obstructive process. If, despite the ultrasound, the diagnosis remains doubtful, computed tomography with limited exposure could be considered, focusing the study area from L3 to the pubic branches(17). The sensitivity of this technique is greater than 80%, with a positive predictive value (PPV) close to 90%(12).
Combining these epidemiological, exploratory and analytical data, several clinical scores have been created for diagnosis: the Alvarado scale, the Samuel M PAS scale (Pediatric Appendicitis Score) (Table II)(18) and, more recently, the pARC(13), the risk calculator for pediatric appendicitis, which includes as variables: sex, age, duration of symptoms, abdominal guarding, pain migration, tenderness in the right lower quadrant and absolute neutrophil count and that, in a prospective study of validation, has shown to surpass the PAS scale as a discriminator of appendicitis in the pediatric age(19).

The treatment of appendicitis is surgical, so children with this suspicion should be evaluated by a pediatric surgeon as soon as possible. Randomized studies recommend the laparoscopic approach compared to the open approach, as it generates a shorter hospital stay, lower risk of surgical wound infection and fewer postsurgical abscesses(20). While waiting for the intervention, the patient will be kept ‘nil-by-mouth’, with intravenous fluid therapy at maintenance requirements, or even correcting a possible hydroelectrolyte imbalance due to dehydration. It will be essential to treat the pain early, as well as to evaluate it periodically, using first-line analgesics (paracetamol, metamizole…), progressing to other drugs such as ketorolac or opioids to reduce the pain, if the previous ones are insufficient. Once the diagnosis is established, the administration of appropriate antibiotic therapy is recommended prior to surgery, ensuring at least one dose 1-2 hours before the incision(20). In simple appendicitis (intact wall), antibiotic therapy will have a prophylactic role and no more doses will be required after the intervention. In complicated cases (gangrenous, perforated), antibiotic therapy will be prolonged until: the patient is afebrile, the general condition has improved and the abdominal examination has normalized(21). There are various guidelines, but the most described in the literature are the use of: cefoxitin, amoxicillin-clavulanate, ceftriaxone with metronidazole or piperacillin-tazobactam, the latter being more recommended in case of generalized peritonitis due to perforation.
Post-appendectomy complications are infectious in the short term and mechanical in the long term. Persistent fever, elevation of acute phase reactants or worsening of the abdominal examination should raise suspicion of the formation of an abdominal abscess (5% of cases, more likely in complicated appendicitis and in patients with a body mass index greater than p95)(20). Intestinal obstruction due to flanges occurs in less than 1% of patients undergoing surgery, taking place weeks after the operation.
Intestinal intussusception
It is the most common abdominal emergency in early childhood, with a peak incidence between 4 and 36 months of life(22), being the most common cause of intestinal obstruction in this age group.
It is produced by the introduction of a fragment of intestine into the adjacent segment in an anterograde direction, dragging the mesentery, and producing venous and lymphatic congestion that leads to edema of the intestinal wall, which can progress to complete obstruction, proximal distension, necrosis and perforation. Regarding the location of the invagination: 90% of cases are ileocolic, located at the ileocecal junction; and the remaining 10% are ileoileal, jejunoileal or colocalized. Regarding the cause, 75% of cases are defined as idiopathic, in which an intussusception “head” is not detected or there is no clear pathological trigger. However, viral infections play a role in its pathogenesis, with epidemic peaks of viral gastroenteritis coinciding with more cases of intestinal intussusception. Around 30% of invaginated patients have presented signs of viriasis in the previous weeks, with adenovirus being one of the most related microorganisms(22). Hypertrophy of Peyer’s patches is assumed after these infections, especially in the ileum, rich in lymphatic tissue, which could act as the head of invagination. However, other pathogenic structures can act as a starting point for invagination: a Meckel’s diverticulum, a polyp, a duplication cyst, a tumor, a vascular malformation, a wall hematoma in Shölein-Henoch purpura, etc., especially in older children, in whom we should always have a high index of suspicion to look for a possible cause.
The classic clinical picture would be: an infant who suddenly presents an episode of colic abdominal pain, with inconsolable crying, drawing of the legs towards the abdomen with paleness and vomiting, reproducing every 15-20 minutes, interspersed with periods of normality and clinical stability. An elongated “sausage”-shaped abdominal mass can be palpated in the right lower quadrant, and 50% may have bloody stools, although the traditional sign of “currant jelly” stools that occurs after mixing blood with mucus when the intestinal wall is ischemic is late and infrequent. However, the usual presentation does not include the elements of the triad (pain, mass and blood in stool), which only appear together in less than 15% of patients. As time goes by from the onset of symptoms, lethargy may appear, to the point of being the guiding sign in some patients. For this reason, intestinal intussusception is part of the differential diagnosis of other entities, such as meningoencephalitis or sepsis(22).
Abdominal ultrasound has demonstrated its superiority, both as a diagnostic and therapeutic technique, with a sensitivity and specificity close to 100% with an expert sonographer, in addition to more easily detecting pathological invaginating heads. The most characteristic finding is the “target” or “doughnut” sign (Fig. 1), detecting in a cross section a segment inserted inside another.

Figure 1. Typical ultrasound image of intestinal intussusception.
The abdominal X-ray, today, only plays a role when there is suspicion of perforation, which would require surgical management. The treatment will consist of hydrostatic or pneumatic reduction, depending on whether a serum or air enema is used, always having previously stabilized the patient and correcting possible water depletion, if there are signs of dehydration. Although comparative evidence is still scarce, there seems to be a higher success rate with pneumatic reduction(23). The correction is performed under ultrasound surveillance, checking its resolution in real time. It is a relatively safe technique, but with a perforation rate of 1-4% (especially in children under 6 months of age, patients with long-term symptoms, signs of severe obstruction or the need for high pressures during reduction)(22). Although they are usually kept hospitalized for 12-24 hours for observation after the maneuver and to monitor recurrences, this practice is questioned, since the rates of re-invagination do not differ in uncomplicated cases in the groups that remain admitted and those discharged home.
Mesenteric adenitis
Clinical entity produced by inflammation of the mesenteric lymph nodes, which are concentrated in the lower right quadrant in the abdominal topology, presenting with symptoms of very acute abdominal pain that are part of the differential diagnosis of acute appendicitis or intestinal intussusception. They usually present a history of a viral process in the previous two weeks. Its prevalence has increased, in part due to the generalization and accessibility of ultrasound in the evaluation of children with acute abdominal pathology. It is diagnosed when it shows lymph nodes with a diameter greater than 8 mm, but it is necessary to rule out other pathologies and check that the appendix shows normal morphology. It is a self-limiting entity, although the symptoms can be prolonged (between 1 and 4 weeks, even longer in some cases)(24) and only supportive treatment must be offered: hydration, pain control and monitoring, which sometimes, due to the intensity of the symptoms, may be necessary to perform it in the hospital environment.
Incarcerated inguinal hernia
The permeability of the peritoneum-vaginal duct leads to the exit of intestinal loops into the inguinal canal, causing pain and irritability. Although, in most cases, it can be reduced spontaneously, it may require maneuvers for reduction (incarceration) or, in the worst case, it may not be possible (strangulation). Inflammation of the hernial sac compromises its vascularization, causing wall edema and signs of obstruction, with vomiting and abdominal distention. Usually, a fixed mass with a hard, red and painful consistency can be palpated, which can extend to the scrotum or the labia majora and which, with adequate containment and analgesia, can be reduced(24).
Intestinal obstruction due to adhesions or flanges
In children with bilious or fecaloid vomiting, distension and abdominal pain and those who have a history of having previously undergone surgical interventions, adhesions or fibrous flanges may have developed that generate obstructive symptoms that, as they evolve, can generate: ischemic areas, hypovolemia due to third space, shock and sepsis. The risk described in retrospective series is 1-5% in the 5 years following the operation, with a higher risk in patients who have undergone reoperation, who have suffered peritonitis or in whom the ileum has been affected(24). The key test, in addition to the high index of suspicion based on the history, is the abdominal x-ray, which will show distended loops, and if the patient can remain upright in a standing position, air-fluid levels (Fig. 2). In infants, another option is the horizontal ray. The initial treatment is to keep them nil-by-mouth, decompress with a nasogastric tube and administer intravenous fluids. If there is no improvement or there is evidence of intestinal ischemia, the treatment will be surgical.
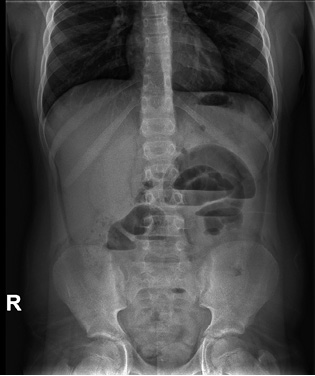
Figure 2. Simple abdominal x-ray, performed in a standing position, in a child with intestinal obstruction. The characteristic air-fluid levels are visible.
Volvulus
During intestinal development in the embryonic stage, an interruption may occur that causes malrotation, predisposing it to turn, compromising vascularization and causing intestinal obstruction. 75% of malrotated newborns will volvulate in their first month of life, especially in the first week(24). It usually presents with abrupt symptoms (abdominal pain, acidosis, shock and bloody stools, with abdominal distension 3-6 h after the onset of symptoms)(25). However, in some children it may present with incomplete or intermittent subocclusions that explain a subacute course.
Ileitis in a patient with multisystem inflammatory syndrome (PIMS) after SARS-CoV2 infection
As already mentioned, a history of having had SARS-CoV2 infection can also guide the patient’s diagnosis. The definition of multisystem inflammatory syndrome (PIMS), after acute infection by this virus, allowed us to identify its expressiveness in terms of abdominal symptoms (60% of PIMS cases)(26), which sometimes, due to their intensity, could resemble an acute abdomen. The following symptoms are especially common: terminal ileitis, ileocolitis(27,28) and mesenteric adenitis, all of them usually non-surgical conditions, although cases of acute appendicitis have also been described in the context of this clinical picture, especially in ages outside the usual epidemiological ranges(26).
Acute gastroenteritis
Finally, a much more common clinical picture than the previous ones, is included in this review as it must always be considered in the differential diagnosis. Fever and intense colicky abdominal pain prior to the onset of diarrhea are characteristic. There are some specific microorganisms such as Yersinia enterocolitica, which usually locate the pain in the right iliac fossa, mimicking appendicitis(24).
Role of the Primary Care pediatrician
The role of the Primary Care pediatrician is the initial diagnostic guidance of the child with acute abdominal pain. To do this, he will take a detailed history, a meticulous examination and assess the need for referral or a specific complementary test.
Conflict of interest
There is no conflict of interest in the preparation of the manuscript. Declaration of interests: none.
Bibliography
The asterisks show the interest of the article in the authors’ opinion.
1.* Banerjee R, Prasad A, Gupta S. Clinical spectrum of acute abdomen in children admitted to pediatric emergency deparment: A prospective study. Curr Med Res Pract. 2019; 9: 49-52.
2.** Hort J. Abdominal pain. In: Cameron P, Browne GJ, Dalziel S and Craig S, eds. Textbook of paediatric emergency medicine 4ª edition. Elsevier Limited; 2023. p. 14752.
3.** Alonso Cadenas JA, de la Torre Espí M. Diagnóstico y tratamiento del dolor abdominal agudo (abdomen agudo) en Urgencias. Diagnosis and treatment of acute abdominal pain (acute abdomen) in the emergency department. Protoc diagn ter pediatr. 2020; 1: 197-213.
4. Maclin J. Acute Abdominal Pain. In: Kline M, ed. Rudolph’s pediatrics 23rd ed. McGraw Hill Ed; 2018. p. 1463-7.
5. Muñoz-Santanach D, Luaces Cubells C. Dolor abdominal agudo. Acute abdominal pain. Pediatr Integral. 2019; XXIII: 15-24. Available in: https://www.pediatriaintegral.es/publicacion-2019-01/dolor-abdominal-agudo/.
6.* García Salido A, De Carlos Vicente JC, Belda Hofheinz S, Balcells Ramírez J, Slöcker Barrio M, Leóz Gordillo I, et al. Severe manifestations of SARS-CoV-2 in children and adolescents: from COVID-19 pneumonia to multisystem inflammatory syndrome: a multicentre study in pediatric intensive care units in Spain. Crit Care. 2020; 24: 666-78.
7.* Boybeyi-Turer O, Ozsurekci Y, Gurlevik SL, Oygar PD, Soyer T, Tanyel FC. Management of acute abdomen during the active disease course of COVID-19 and multisystem inflammatory syndrome in children. Surgery Today. 2022; 52: 1313-9.
8.* Monterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database Sys Rev. 2011; 19: CD005660.
9. Almaramhy HH. Acute appendicitis in young children less than 5 years: review article. Ital J Pediatr. 2017; 43: 15-23.
10. Le Coz J, Orlandini S, Titomanlio L, Rinaldi VE. Point of care ultrasonography in the pediatric emergency department. Ital J Pediatr. 2018; 44: 87-94.
11. Lipsett SC, Bachur RG. Current Approach to the Diagnosis and Emergency Department Management of Appendicitis in Children. Pediatr Emerg Care. 2017; 33: 198-203.
12.** Baykara AS. Acute Appendicitis in Children: Evaluation of the Diagnostic Efficacy of Ultrasonography and Computed Tomography. Cureus. 2023; 15: e43860. Available in: https://doi.org/10.7759/cureus.43860.
13. Brandt ML, López ME. Acute appendicitis in children: Clinical manifestations and diagnosis. In: UpToDate. 2022. Available in: https://uptodate.com.
14.* Echevarria S, Rauf F, Hussain N, Zaka H, Farwa U, Ahsan N, et al. Typical and Atypical Presentations of Appendicitis and Their Implications for Diagnosis and Treatment: A Literature Review. Cureus. 2023; 15: e37024.
15. García Camiño E, Campillo i López F, Delgado Díez B, Ballesteros Moya E, Calle Gómez A, Martín Sánchez J. Appendicitis in children under four years. Identifying signs, symptoms, laboratory and imaging parameters for an early diagnosis. Rev Pediatr Aten Primaria. 2014; 16: 213-8.
16. Peña L, Beltrá R. Dolor Abdominal Agudo. Acute abdominal pain. Chapter 283. In: Moro M, Málaga S. Tratado de Pediatría Cruz. 11th ed. 2014. Ed. Médica Panamericana.
17. Taylor GA, Brandt ML, López ME. Acute appendicitis in children: Diagnostic imaging. In: UpToDate. 2022. Available in: https://uptodate.com.
18.* Samuel M. Pediatric appendicitis score. J Pediatr Surg. 2002; 37: 877-81.
19.* Cotton DM, Vinson DR, Vázquez Benítez G, Warton EM, Reed ME, Chettipally UK, et al; Clinical Research on Emergency Services and Treatments (CREST) Network. Validation of the Pediatric Appendicitis Risk Calculator (pARC) in a Community Emergency Department Setting. Ann Emerg Med. 2019; 74: 471-80.
20. Brandt ML, López ME. Acute appendicitis in children: Management. In UpToDate. 2023. Available in: https://uptodate.com.
21. Lee SL, Islam S, Cassidy LD, Abdullah F, Arca MJ; 2010 American Pediatric Surgical Association Outcomes and Clinical Trials Committee. Antibiotics and appendicitis in the pediatric population: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee systematic review. J Pediatr Surg. 2010; 45: 2181-5.
22. Salazar JH. Intussusception in children. In: UpToDate. 2023. Available in: https://uptodate.com.
23.** Gluckman S, Karpelowsky J, Webster AC, McGee RG. Management for intussusception in children. Cochrane Database Syst Rev. 2017; 6: CD006476.
24. Neuman MI. Causes of acute abdominal pain in children and adolescents. In: UpToDate. 2022. Available in: https://uptodate.com.
25.** Laje, P. Abdominal Surgical Emergencies in neonates. Neoreviews. 2023; 24: e97-e106. Available in: https://doi.org/10.1542/neo.24-2-e97.
26. Rouva G, Vergadi E, Galanakis E. Acute abdomen in multisystem inflammatory syndrome in children: A systematic review. Acta Paediatr. 2022; 111: 467-72. Available in: https://doi.org/10.1111/apa.16178.
27. Rico C, Souto H, Espinosa Góngora R, Espinoza Vega ML, Alonso Calderón JL. Acute abdomen in COVID-19 disease: the pediatric surgeon’s standpoint. Cir Pediatr. 2021; 34: 3-8.
28.* García Salido A, Antón J, Martínez Pajares JD, Giralt García G, Gómez Cortés B, Tagarro A. Documento español de consenso sobre diagnóstico, estabilización y tratamiento del síndrome inflamatorio multisistémico pediátrico vinculado a SARS-CoV-2 (SIM-PedS). Spanish consensus document on diagnosis, stabilization and treatment of pediatric multisystemic inflammatory syndrome linked to SARS-CoV-2 (SIM-PedS). An Pediatr (Barc). 2021; 94: 116.e1-e11.
Recommended bibliography
– Hort J. Abdominal pain. In: Cameron P, Browne GJ, Dalziel S and Craig S, eds. Textbook of pediatric emergency medicine 4th edition. Elsevier Limited; 2023. p.14752.
It is the chapter dedicated to acute abdomen in a practical and updated pediatric emergency book. We especially highlight the examination section.
– Alonso Cadenas JA, de la Torre Espí M. Diagnóstico y tratamiento del dolor abdominal agudo (abdomen agudo) en Urgencias. Diagnosis and treatment of acute abdominal pain (acute abdomen) in the emergency department. Protoc diagn ter pediatr. 2020; 1: 197-213.
A useful and well-structured protocol, with practical information for emergency care and analysis of the most relevant quality care indicators.
| Clinical case |
|
A 7-year-old boy attends his Health Care Center for re-evaluation of abdominal pain. Yesterday, he was already evaluated when mild-moderate pain began in the mesogastrium, without other alarm signs and with a normal abdominal examination. Since then, he has vomited twice, has not had pathological bowel movements, and the pain has intensified in the last few hours, migrating to the right lower quadrant. He also reports some discomfort when urinating. The child’s general condition is affected, he looks in pain, he cannot get on the stretcher without help, and he is pale. His abdomen is a little distended, manifesting defense on palpation, and the pain worsens when suddenly decompressing the right iliac fossa during palpation.
|