Gynecological examination and most common abnormalities of the menstrual cycle in adolescence
Gynecological examination and most common abnormalities of the menstrual cycle in adolescence  |
| Topics on Continuous Training |
M. Guerrero Ibáñez, M. Franco Horta, J. Martínez-Guisasola Campa
Department of Obstetrics and Gynecology for Children and Adolescents. Burgos University Hospital
| Abstract
The main aim of this article is to review the most frequent reasons for consultation related to disturbances of the menstrual cycle in the pediatric and adolescent age group. During their transition through puberty and especially in its first years, disorders of menstruation become the most common complaint requiring the attention of the gynecologist, including problems such as amenorrhea, dysfunctional uterine bleeding and dysmenorrhea. The immaturity of the hypothalamus-pituitary-ovary (HPO) axis with its associated anovulation, are involved in a high proportion of the episodes. Dysmenorrhea is another common reason for consultation due to its impact on the quality of life in the young female, making its adequate treatment essential. Primary amenorrhea is strongly associated with genetic diseases and endocrine disorders so it is important to achieve the diagnosis as early as possible. Moreover, the relevance of history taking and physical examination must be highlighted as they provide a crucial approach to the underlying diagnosis. |
| Resumen
El objetivo principal de este artículo es una actualización orientada a la práctica diaria sobre los motivos de consulta más frecuentes relacionados con las alteraciones del ciclo menstrual en la etapa puberal y en la adolescencia. Durante la transición a la pubertad y en los primeros años de esta, las alteraciones del ciclo menstrual, desde la amenorrea al sangrado menstrual frecuente o infrecuente, son uno de los principales motivos de consulta en Ginecología. En un alto porcentaje de jóvenes, están relacionadas con la propia inmadurez del eje hipotálamo-hipófisis-ovario (HHO) y la anovulación asociada. La dismenorrea es otro motivo de consulta habitual por la repercusión en la calidad de vida que puede tener en la joven, y es fundamental su tratamiento adecuado. Las amenorreas primarias presentan una elevada asociación con patología genética y endocrina, por lo que deben ser diagnosticadas de manera temprana. Además, queremos destacar la importancia de una adecuada anamnesis y exploración física general y ginecológica en la orientación diagnóstica de estos cuadros. |
Key words: Adolescence; Gynecological examination; Menstrual cycle; Amenorrhea; Dysmenorrhea.
Palabras clave: Adolescencia; Exploración ginecológica; Sangrado menstrual; Amenorrea; Dismenorrea.
Pediatr Integral 2022; XXVI (5): 270 – 279
OBJECTIVES
• To carry out a specific history taking to assess the existence of abnormalities of the menstrual cycle, and recognize the circumstances that may favor communication with the girl or adolescent.
• To know how to carry out the gynecological examination in girls and adolescents and the environment that can favor its performance.
• To identify situations that meet the criteria for primary and secondary amenorrhea and start an etiological study.
• To recognize the adolescents with heavy menstrual bleeding and carry out the most appropriate treatment for each clinical situation.
• Diagnosis and treatment of primary dysmenorrhea.
• To identify premenstrual syndrome and the premenstrual dysphoric disorder.
|
|
|


Gynecological examination and most common abnormalities of the menstrual cycle in adolescence
Gynecological examination
Introduction
The request for attention in the Child and Adolescent Gynecology consultation is increasing, due to the appearance of certain signs or symptoms that, on occasions, generate confusion between the physiology and the pathology of pubertal development, and require a more specific study; but, on other occasions, this demand is related to the lack of knowledge of the wide variability of the physiology of puberty and the development of girls and adolescents; and in others, it is produced by the current social and family pressure to study the physiology in depth to rule out pathology outright.
History taking
Empathy and proximity are essential in the interview. Family history is particularly important due to its hereditary burden, especially in female relatives.
The chronological age of the patients who attend the Child and Adolescent Gynecology consultation is variable. Young girls require the support of a parent, both for the history taking and for the examination, in which case the presence of this adult figure is essential and accompanies them at all times. In the case of young adolescents or if the existence of sexual abuse is suspected, it is advisable to reserve a time and space for a one-to-one interview with the patient, where she feels comfortable and where the confidentiality of the data provided is ensured. Obtaining these data is essential for diagnosis and/or subsequent treatment.
Whenever possible, depending on age, it is important that the patient communicates the symptoms herself, since the information transmitted by her or by the family member or companion may be contradictory. It is essential to listen and learn about the girl or young woman’s concerns and experiences, and transmit the importance of knowing her own body as well as current and future changes, and also answering any doubts she may have. Proximity and empathy, but without paternalism, are necessary for the correct development of the consultation(1,2).
After identifying the reason for the consultation, the existence of a connection between the symptoms presented by the patient and her personal and family background, will be assessed.
The existence of current or previous diseases of special relevance must be inquired, including genetic or chromosomal abnormalities that may condition development, oncological processes with radiotherapy or chemotherapy that may affect ovarian reserve(3) and abdominal surgeries, especially pelvic or lower genital tract surgeries or medication intake that may interfere with the normal functioning of the hypothalamus-pituitary-ovary (HPO) axis. In young women, they should be asked about the consumption of toxic substances and informed about their repercussion on health, advising towards their discontinuation.
In the case of secondary amenorrhea, relevant factors include emotional, physical or nutritional stress(3,4), which inhibit the HPO axis by increasing cortisol secretion and suppressing reproductive function, with subsequent amenorrhea as a functional adaptive response. It is advisable to assess the existence of: mood swings, adaptation problems at school or work, academic stress, problems with family member/s or with other relationships… Changes in eating habits that lead to loss or gain are in a short period of time become of special relevance, since they also interfere with the functioning of the axis, especially those related to eating behavior disorders, as well as intense physical activity carried out by high-competition athletes. In our experience, we have particularly observed this situation among dance students, as, in addition to the daily practice of intense physical exercise, they sometimes associate a restrictive eating behavior.
If the adolescent has already presented menarche, the time elapsed since that date should be known, since menstrual irregularities are frequent during the first 2-3 years after menarche(1,3). Other important data are the menstrual pattern (MP: number of bleeding days/interval, between the start of a bleeding cycle and the onset of the following one), to assess the existence of alterations in the menstrual cycle, either in the amount of bleeding or the cyclicity of it, as well as the last menstrual period (LMP), to identify the moment of the cycle in which the patient is at the time of the examination and make a correct interpretation of the findings. The presence of dysmenorrhea, pain during menstruation, is common in adolescents and will be discussed subsequently. In the event that the patient has or has had sexual relations, it is a good opportunity to advise on contraception and on the prevention of sexually transmitted infections. Additionally, the existence of previous pregnancies should be recognized(1,3).
Taking into account the repercussion that family history can have on heredity and gynecological development, it is important to know the existence of diseases in parents and siblings, especially in female relatives such as mother and sisters, regarding: age of menarche, menstrual disorders and gynecological pathology, existence of coagulation disorders (hypo/hypercoagulability), endocrinological pathology and cases of early or late puberty(1,3).
Gynecological and breast examination
The gynecological examination should be the minimum with which the maximum information is obtained. Sometimes it can be postponed if the patient is not ready for it.
It is necessary to clearly differentiate between the examination and assessment of pediatric girls, especially the youngest ones, and the examination of young adolescents. Gynecological examination in pediatric patients is generally reduced to situations to: rule out pathology of the genital tract, diagnose gynecological infections or assess the presence of intravaginal foreign bodies. Consultation for genital bleeding or to assess the existence of sexual abuse is less frequent. The examination in the pediatric age generates fear and restlessness in the girl, thus it is preferable to be carried out with a companion who, in most cases, collaborates with the examination, unless the patient demands otherwise. Proximity is important, explaining the examination that is going to be carried out in understandable terms, the objective of each action and allowing time for the patient to be prepared for its performance(5). Sometimes, it may not be essential to perform the examination at that time, or the patient is not prepared for it, so it may be postponed until the situation is more favorable. The gynecological examination should be the minimum with which the maximum information is obtained(2).
To perform a complete examination, it is also necessary to obtain an assessment of: body mass index, blood pressure, thyroid gland, lymph nodes, breast development, abdomen, skin and skin appendages.
Placement of prepubertal girls and young women for an adequate gynecological examination
For the examination to be effective, it is important to adapt it to the age of the patient.
A clear, concise and simple explanation of the examination to be carried out can facilitate the calmness and cooperation of the patient.
In the case of girls under 4 years of age, they can be placed on the family member’s knees, placing the girl’s legs astride the adult’s thighs (Fig. 1A). Another option consists of placing the patient on a stretcher in the supine position with the hips abducted and the feet together, like a frog (Fig. 1B). Another alternative for the examination consists of placing the patient with her thighs close to her chest, raising the buttocks and hips (Fig. 1C), thus allowing the lower part of the hymen to be seen, the lower part of the vagina, and sometimes, the upper part of the vagina and the cervix, but as an inconvenience visual contact with the patient is lost.
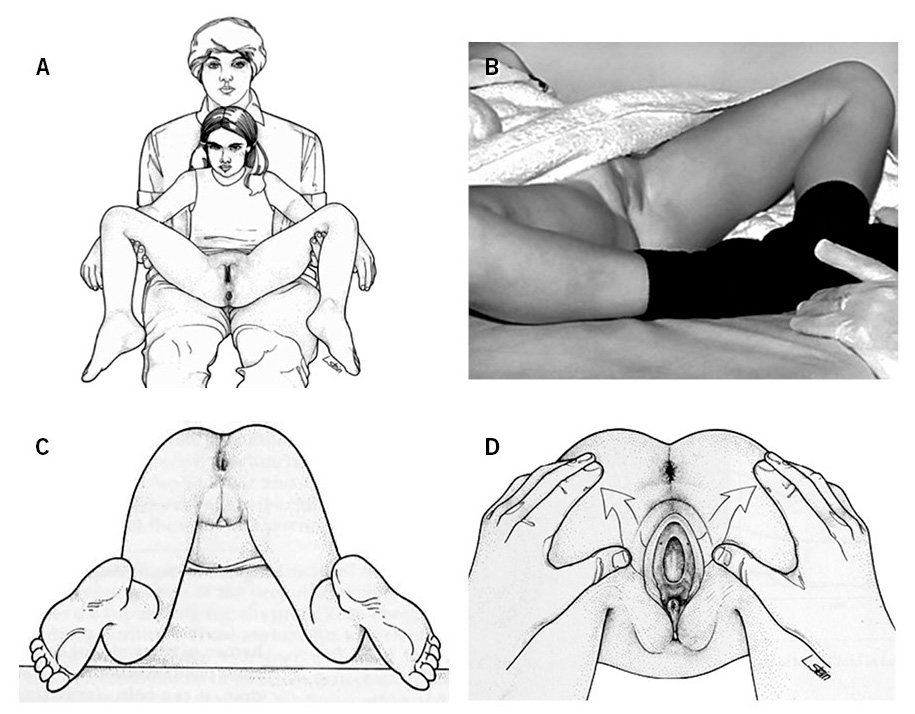
Older patients may prefer to use stirrups on the gynecological examination table, trying to get the patient in a position that allows constant eye contact during the examination. In the event that the patient has had sexual intercourse, the examination will be carried out in the same way as in young women, by inspecting the lower genital tract and visualizing the vagina and cervix using virginal specula.
Carrying out the gynecological examination with the patient alone is usually recommended, as long as she is over 13 years of age or if she is younger and requests it(1). A time for intimate dialogue should be reserved for the adolescent to pose questions that she has not asked in the presence of her companion, especially those related to the sexual sphere, or to raise that possibility on our part if it has not been done before and offer advice about contraception and sexually transmitted infections (Table I).

Breast inspection and examination is essential in cases of abnormalities in pubertal development, suspicion of malformations or asymmetry. The initial development of the breast can be uncomfortable and the examination can be painful, without this implying pathology. Palpation is important, especially in obese girls to assess for the presence of breast tissue that may lead to misstaging of Tanner stages. The development of the breast bud can be asymmetric and there can be up to 12 months of difference between the beginning of the development of one breast and that of the other(1).
At the end of the examination, regardless of the age of the girl or young person, it is important to inform her of our diagnosis or suspected diagnosis, addressing her in understandable language and engaging in conversation with her, involving her in the information so that she understands it and carries out opportune questions.
In the elaboration of the final report on the gynecological and breast examination, especially in the case of a study of pubertal development, the pubertal stage must be referenced according to the Tanner stages(6), which is essential if the follow-up is carried out by several specialists to objectively assess its progression (Fig. 2).
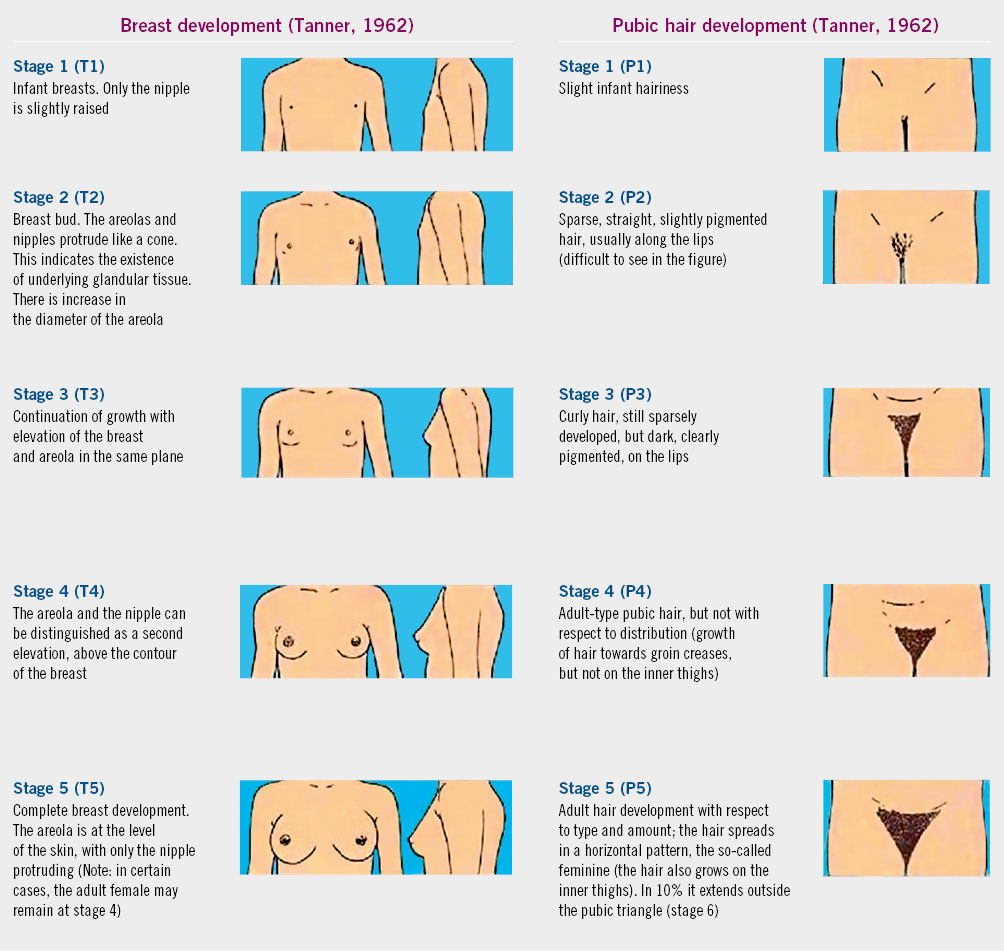
Figure 2. Pubertal Tanner stage in girls. Taken from: Tanner JM. Growth at adolescence. 2nd ed. Oxford: Blackwell; 1962.
Complementary examinations
Gynecological ultrasound is essential in the study of the internal genital tract.
When the internal genital apparatus must be evaluated for a diagnosis during consultation, gynecological ultrasound has become a basic and fundamental exploration due to its innocuousness, easy accessibility and the immediacy and relevance of the information. The exploration routes will depend on the age of the patient, so that transabdominal route with bladder repletion is used in girls or young females who are not sexually active, whereas intravaginal is reserved for sexually active adolescents. In cases in which it is not possible to visualize the internal genital apparatus through the aforementioned routes, transrectal or transperineal ultrasound can be used(1,7).
It is important to know the differences in the anatomy of the internal genital tract in the prepubertal and postpubertal stages (Table II).

If a nodule or the presence of secretions from the nipple (telorrhea) is detected in the breast examination, other complementary examinations may be required, such as: breast ultrasound, cytological study of the secretions or even breast puncture for the pathological study of lesions.
Menstrual cycle disturbances
The normal menstrual cycle ranges between 28 ± 7 days, with a bleeding duration of 4-8 days, and a menstrual loss between 30-80 ml per cycle. In adolescence, its alterations affect 75% of young people.
According to the ACOG (American College of Obstetricians and Gynecologists)(8), the identification of menstrual disorders in adolescence is essential to prevent health problems in adulthood. To meet this objective, it is necessary to know the physiology of puberty, to understand the difference between normal and pathological menstruation, considering the menstrual cycle as a vital sign, a reflection of a state of good health.
The normal menstrual cycle ranges from 28 ± 7 days, with a bleeding duration between 4-8 days, the amount of menstrual loss ranges from 30-80 ml per cycle. Some authors propose greater flexibility in adolescents, since 55-82% of cycles are anovulatory in the first 2 years after menarche; between 30-55% between 2-4 years and are even detected in 20% of young women 5 years after menarche(2,3,9,10).
Menstrual cycle disturbances affect a high number of adolescents (75%)(2,3) and are usually secondary to functional disorders, due to immaturity of the HPO axis. They are a common reason for consultation and are usually related to: the absence of menstruation (primary or secondary amenorrhea), the interval between cycles (frequent, infrequent or irregular menstrual bleeding), heavy menstrual bleeding, as well as the presence of pain during menstruation (dysmenorrhea).
Amenorrhea
Amenorrhea or absence of period should be studied. Secondary amenorrhea, of endocrine or functional cause, is more frequent. In the presence of primary amenorrhea, anomalies of genital development must be ruled out.
The absence of periods can be primary or secondary. Primary amenorrhea is defined as the absence of a period at 16 years of age in the presence of secondary sexual characteristics, or at 14 years of age in the absence of secondary sexual characteristics. 60% of cases are due to genetic abnormalities that affect genital development, and 40% to endocrine disorders. Secondary amenorrhea is defined as the disappearance of the period for more than 6 months(11).
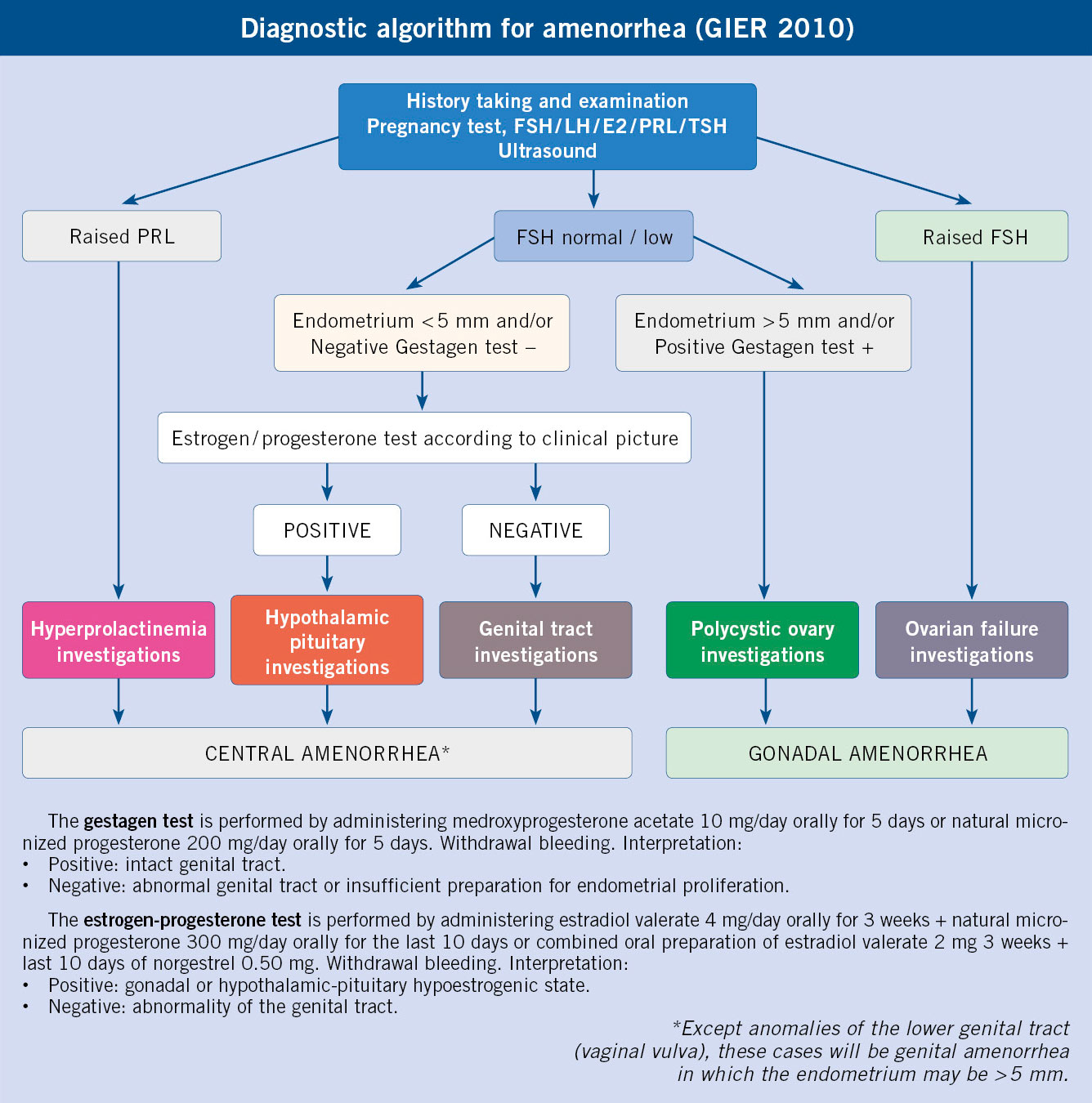
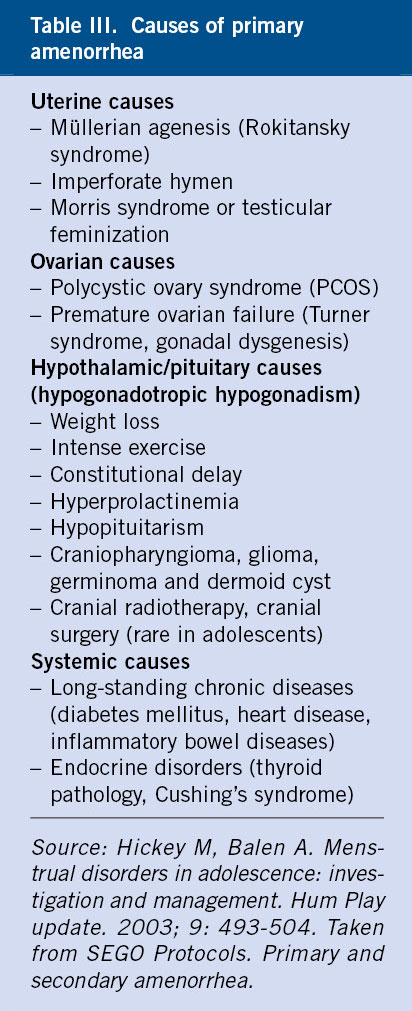
The main causes of amenorrhea are collected in tables III and IV, and they overlap in both types of amenorrhea, although the vast majority are reduced to the diagnoses of: polycystic ovary syndrome (PCOS), hyperprolactinemia, premature ovarian failure (POF) and hypothalamic amenorrhea.

The Reproductive and Endocrinology Interest Group (Grupo de Interés de Endocrinología Reproductiva [GIER]) for the diagnosis of amenorrhea, established in 2010 a classification of amenorrhea based on the anatomical etiology area and, in this way, they were classified as: central (hypothalamus-pituitary), gonadal (ovaries) or genital (uterus-vagina)(12).
On these bases, a simplified diagnostic algorithm for amenorrhea is proposed.
Primary amenorrhea is less common than secondary amenorrhea and requires a complete study in which the general examination and the staging of pubertal development are especially relevant(3,13).
• Normal pubertal development with normal height and weight, is suspicious for anatomical malformation of the uterus or vagina: hymenal atresia, imperforate hymen, vaginal septum, agenesis of the uterus and/or vagina (Rokitansky syndrome or Morris syndrome or testicular feminization or androgen insensitivity). The gynecological examination must be complemented with ultrasound and/or MRI; sometimes, hormonal study and karyotype are required.
• Pubertal delay: temporary pubertal delay, hypothalamic-pituitary failure (hypogonadotropic hypogonadism) or peripheral failure (hypergonadotropic hypogonadism). Complementary studies to be requested based on evolution. It is important to assess progression using the Tanner stages.
• Infantilism: absence of sexual development by the age of 15-16 years (Tanner stage I). Hormonal determinations, radiological exams of the brain (X-ray, CT, MRI) and chromosomal analysis are necessary. The cause may be central: pituitary tumors (prolactinoma or craniopharyngioma) or of hypothalamic origin (Kallman syndrome) or gonadal, gonadal dysgenesis that occurs with primary ovarian insufficiency (chromosomal, it is important to make the diagnosis of chromosomopathy associated with the presence of Y chromosome) or secondary to oncological treatments (chemo or radiotherapy).
• Infantilism and low weight: assess body image disorders (anorexia and bulimia) or by history taking, high performance athletes, with important daily discipline and dietary control.
• Virilization and/or hirsutism: complement the examination and ultrasound with androgen concentrations and karyotype. Etiological suspicion of: adrenal hyperplasia, virilizing tumors and chromosomal alterations associated with the presence of the Y chromosome.
In all cases of primary amenorrhea the treatment is etiological, hence, the responsible cause must be treated.
Secondary amenorrhea is much more frequent than primary amenorrhea and the most common causes in adolescence are related to: physical or psychological stress, eating disorders and their effect on weight, intense physical exercise (competition athletes, dance students…) and polycystic ovary syndrome (PCOS). Always, before starting the secondary amenorrhea study, if the adolescent has sexual intercourse, the possibility of pregnancy should be assessed(2,4,10,11).
History taking, physical examination, hormonal study and gynecological ultrasound are usually the most used tests to reach the diagnosis.
Hypothalamic stress amenorrhea is suspected after a directed history, in which the adolescent refers to a personal stage of restlessness or worry, or the performance of intense physical activities. In eating behavior disorders, it may be that the adolescent does not verbalize it, but the family does, or it may be suspected after calculating the BMI. In hypothalamic amenorrhea, ultrasound shows no pathology and hormonal analysis shows hypoestrogenism secondary to lack of gonadotropic stimulation. Treatment is etiological, although in some situations of eating disorders, if amenorrhea persists over time after weight regain, it may be necessary to establish hormone replacement therapy(11).
Polycystic ovary syndrome (PCOS) has a prevalence between 8-26% in adolescence. It can present itself in many ways: infrequent menstrual bleeding, clinical hyperandrogenism (acne and/or hirsutism, of variable intensity) and, occasionally, obesity or overweight. Typical hormonal laboratory tests reflect anovulation and hyperandrogenism and, in some cases, insulin resistance. Ultrasound aids diagnosis, especially if the ovaries have the characteristic appearance. Treatment must be individualized. If there is clinical hyperandrogenism, combined hormonal therapy with antiandrogenic progestins (cyproterone acetate, dienogest, or drospirenone) or spironolactone may be necessary. In cases of insulin resistance, the use of insulin-sensitizing drugs (metformin®) may be indicated and, in cases where there is a high BMI, weight loss and physical exercise are essential(3,10,11).
Premature ovarian failure (POF) is diagnosed as hypergonadotropic hypogonadism and no ovarian follicles are visualized on ultrasound. It causes a significant impact on the health and reproductive future of adolescents, as well as an increase in mortality of up to two times. The association should be considered, especially in patients who have received oncological treatments (alkylating agents and/or pelvic radiotherapy). The treatment will be hormone replacement therapy with the use of estrogens and gestagens(3,11).
Heavy menstrual bleeding
Heavy menstrual bleeding (HMB) is common in adolescence, as it is related to the immaturity of the HPO axis and anovulation. It is a common cause of anemia in adolescents.
The American Academy of Pediatrics (AAP) recommends considering menstruation at routine visits as one more vital sign. It must be taken into account that, in the first year after menarche, menstruation should not have a frequency of less than 45 days. With age, menstruation becomes regular; in the third year after menarche, the period is usually 21-35 days, with a duration of menstruation of 3-7 days. Normally, the cycle length of an adolescent is established at 19-20 years of age(14).
Heavy menstrual bleeding (HMB) can be prolonged in duration, abundant in quantity or irregular in nature, and it occurs without being related to a systemic pathology or an anatomical substrate. In most cases, the problem lies in an immaturity of the HPO axis that causes anovulation, and produces HMB on the base of a proliferative endometrium that does not have the stabilizing action of the progesterone produced at ovulation(15).
Irregular bleeding, particularly that caused by anovulation, can be prolonged and heavy. However, in patients with regular and cyclical menstruation who present with prolonged and/or heavy bleeding, a haematological cause should be suspected. Von Willebrand disease and coagulation disorders may account for 13 and 44%, respectively, of patients with menstrual bleeding heavy enough to warrant hospitalization(16).
In the study of HMB it is important to ask about: episodes of epistaxis, ecchymosis or excessive bleeding during any surgery, as well as a family history that reveals any coagulation, liver (coagulation factors and estrogen metabolism) or kidney disorders that may interfere with platelet function. It is known that a decrease in glomerular filtration produces an elevation in prolactin that leads to anovulation. In addition, there are autoimmune diseases, such as lupus or juvenile rheumatoid arthritis, which have been more frequently associated with dysfunctional bleeding(17,18).
In sexually active patients, the possibility of an infectious etiology that conditions a pelvic infection, such as that caused by Chlamydia or Gonococcus, must be taken into account. Much less frequently at this stage, may the etiology be related to the existence of endometrial polyps that can be assessed by gynecological examination(19).
Treatment is determined by the severity of the case. In mild cases, a diet rich in foods with iron or iron intake is recommended, and assessment of cycles using a menstrual calendar, in order to know the pattern of bleeding in subsequent cycles. NSAIDs have been shown to be more effective than placebo in controlling menstrual bleeding, while improving dysmenorrhea, if it coexists. If there is no therapeutic response or if it is inadequate, tranexamic acid (Amchafibrin® 500 mg), an antifibrinolytic that acts by interrupting the coagulation cascade, can be used: 1 g/6-8 h orally, for 3-5 days, until 22 g total dose is reached. It reduces bleeding by 40-50% in patients with HMB and can be administered together with combined hormonal treatment(20). In severe or prolonged cases in which bleeding is not controlled with antifibrinolytics, and with systemic repercussions, combined hormonal treatment is started with 1 tablet/12 h until it stops, subsequently maintaining treatment with 1 tablet/24 h for a period of time, either continuously or following a cyclical pattern. It is possible to use treatment with gestagens in case estrogens are contraindicated, or to add gestagens in the second part of the cycle sequentially. In rare cases where combined hormone therapy at 1-2 tabs/day does not control bleeding, hormone therapy may be increased to 3-4 tabs/day with gradual tapering over the next 2 weeks. In severe cases, patients with continuous bleeding, syncope or dizziness, as well as those whose hemoglobin is <7-8 g/dl, will require hospital admission(20-22).
Dysmenorrhea
Dysmenorrhea has a negative effect on the quality of life of adolescents, affecting their personal development. It is related to ovulation. It generally responds well to NSAIDs.
Dysmenorrhea is defined as pain that precedes and/or accompanies menstruation, of variable intensity and accompanying symptoms (headache, diarrhea, nausea, vomiting, dizziness…), but which can interfere with quality and normal life habits, such as attending school or other activities. It can affect 20-60% of the adolescent population according to various authors, with cases of severe and limiting involvement being 10-15%(2,10,23).
Dysmenorrhea is classified as primary or secondary. Primary dysmenorrhea is the most frequent form of presentation in adolescents. The pathophysiology is related to the postovulatory period: after ovulation, the decrease in progesterone induces the synthesis of prostaglandins at the endometrial level, which produce vasoconstriction, ischemia and pain at the uterine level, and smooth muscle contraction, thus explaining the coexistence of other accompanying gastrointestinal symptoms. In general, it does not usually coincide with menarche, but appears later, when the menstrual cycles begin to be ovulatory.
Secondary dysmenorrhea has its origin in other underlying pathologies, anatomical alterations or pelvic infections. In the case of adolescents, the most frequent cause of secondary dysmenorrhea is endometriosis(24).
The treatment of primary dysmenorrhea should be aimed at reducing the excess of prostaglandins, with NSAIDs being the first therapeutic step, the intake of which should be started one day before the onset of menstruation. If pain persists despite treatment with optimal doses of NSAIDs or if contraception is required, hormonal therapy can effectively improve dysmenorrhea (Table V). In the case of secondary dysmenorrhea, the treatment will be etiological.

Premenstrual dysphoric disorder and premenstrual syndrome
Mood disturbances related to the menstrual cycle are not common in adolescence. The need for hormonal or antidepressant treatment will be assessed.
Premenstrual dysphoric disorder (PMDD) occurs in 2-6% of menstruating women worldwide and has been included in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5). PMDD is included within depressive disorders and its characteristic entails its moment of presentation in relation to the menstrual cycle. Symptoms of anxiety and depressed mood begin in the second phase of the cycle, after ovulation, with significant improvement when menstruation occurs. This entity produces general malaise and significant functional impairment, and can also be accompanied by physical and behavioral symptoms. It is important to differentiate between PMDD and premenstrual syndrome (PMS), which has a much higher incidence, around 30% of adolescents, and it does not have the same repercussion or seriousness at an affective level. Almost half of the patients who report symptoms that fall within PMS do not meet diagnostic criteria for PMDD(25).
More data is needed to support the efficacy of hormonal contraceptive methods as a treatment for PMS, especially in adolescents, but it is true that some experts recommend this treatment if, in addition, they are patients who suffer from dysmenorrhea or need contraception. In the case of severe PMS and PMDD, there is evidence that the use of serotonin reuptake inhibitors (SSRIs) constitutes the first line of treatment in adult women. They have a rapid onset of action, so they can be prescribed continuously or intermittently, beginning with ovulation (or with the onset of symptoms in the luteal phase) and stopping when symptoms subside. The treatment indicated in adolescents is the same as in the adult population, for example: fluoxetine 20 mg/day orally.
Role of the Primary Care pediatrician
The Primary Care pediatrician establishes contact with his patients from the first days of life, so he has the advantage of having a close relationship with them and their families. The control of growth and development that he carries out over the years offers him the possibility of being able to detect alterations in the pubertal development of the girl at the beginning of adolescence. It is essential to know the chronology of pubertal development and its possible variations, and the association that certain systemic diseases or genetic or chromosomal abnormalities may present with alterations in pubertal development or the menstrual cycle, to suspect the existence of pathology in the progression of puberty.
If menarche has not occurred by 14 years of age with the absence of secondary sexual characteristics or by 16 years of age with their presence, it is necessary to refer for an endocrinological and/or gynecological assessment due to primary amenorrhea. Delaying referral is not recommended, as it is highly associated with the existence of pathology, except in cases of developmental and constitutional delay, in which case there is a family history. Menstrual cycle disturbances are very common in the first years after menarche, especially during the first one, so in their presence, the adolescent and family must be reassured, informing that as the HPO axis matures it will resolve without requiring treatment in most cases. In case of prolonged amenorrhea or if they are accompanied by clinical signs of hyperandrogenism, it is advisable to refer to the Endocrinology and/or Gynecology consultation due to a high suspicion of ovarian or adrenal pathology. It is necessary to take into account the influence that physical or psychological stress can have on the menstrual cycle and investigate its possible relationship.
In cases in which the alterations of the menstrual cycle are due to excess, it is necessary to assess whether they meet the criteria for heavy menstrual bleeding, carry out analyzes and from Primary Care initiate the treatment of those of mild intensity and follow up. Most of the clinical pictures are related to anovulation and will resolve with maturation of the HPO axis. Cases of more severe intensity with clinical or analytical repercussions, those that do not show improvement after treatment with NSAIDs or antifibrinolytics, or those that are prolonged over time, require more specific studies and treatments.
Dysmenorrhea is a frequent symptom in adolescence, more typical time after menarche, since it is related to the presence of ovulatory cycles. It usually presents a good response to treatment with different NSAIDs. In cases of severe dysmenorrhea or those that do not show improvement with an adequate pattern of analgesia, it is recommended to perform a gynecological evaluation to rule out organic pathology. Severe cases present a good response to hormonal therapy.
PMS is not frequent in adolescence, but from Primary Care its diagnosis can be suspected in the presence of anxious or depressive symptoms directly related to the post-ovulatory stage and that improve after menstruation. In severe cases, it may be necessary to start hormone therapy or SSRI, so referral to Gynecology or Psychiatry should be considered.
Conflict of interest
There is no conflict of interest in the preparation of the manuscript.
Bibliography
The asterisks reflect the interest of the article according to the authors.
1.*** Protocolos SEGO. Sociedad Española de Ginecología y Obstetricia. Entrevista y exploración en ginecología en la adolescencia. Last update: January 2013. Gynecological history-taking and physical examination in adolescents. Prog Obstet Ginecol. 2014; 57: 375-9. Available at: http://dx.doi.org/10.1016/j.pog.2014.05.003.
2.** Curell Aguilà N, Parera Junyent N. Exploración ginecológica de la adolescente. Trastornos del ciclo menstrual (sangrado infrecuente o ausente, sangrado excesivo, dismenorrea). Adolescere. 2019; VII: 6-15.
3.*** Rodríguez Jiménez MJ, Curell Aguilá N. El ciclo menstrual y sus alteraciones. Pediatr Integral. 2017; XXI: 304-11.
4.* Mancini F, Martínez F, Tur R. Estudio y tratamiento de las amenorreas hipotálamo-hipofisarias. Prog Obstet Ginecol. 2017; 60: 495-504.
5.*** Ginecología Pediátrica. Documentos de Consenso SEGO 2017. Coordinador: Cancelo Hidalgo MJ. Miembros: Parera i Junyent N, Almansa González C, Rodríguez Jiménez MJ, Hernández de la Calle I.
6.* Tanner JM. Growth at adolescence. 2nd ed. Oxford: Blackwell; 1962.
7.* Avilés Vistorte Y, Tallón Guerola P, Calabuig Barbera E, Rojas Blandón JF. Ecografía ginecológica en la infancia y adolescencia. Radiología. 2016; 58: 1549.
8.* Committee Opinion No. 651 Summary: Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign. Obstet Gynecol. 2015; 126: 1328.
9.* Adams PJ, Menstruation in Adolescents: What’s normal? Medscape J of Med. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2644006/.
10.*** Curell Aguilà N. Normalidad y alteraciones de la menstruación en adolescentes. Pediatr Integral. 2013; XVII: 161-70.
11.*** Protocolo SEGO. Amenorrea primaria y secundaria. Sangrado infrecuente. Update: February 2013. Protocolo SEGO. Primary and secondary amenorrhea. Infrequent bleeding. Prog Obstet Ginecol. 2013; 56: 387-92.
12.* Tur R, Fontes J, Salvador C, Manzanares MA, Herrero J, Graña M, et al. Consenso de Granada del Grupo de Interés de Endocrinología Reproductiva (GIER) para el diagnóstico de las amenorreas. Rev Iberoam Fert Rep Hum. 2011; 28: 35-43.
13.*** Ascaso Matamala AM, Guerrero-Fernández J, Bueno Lozano G, Rodríguez Contreras FJ. Pubertad retrasada. Hipogonadismo en el niño mayor y adolescente. Cap. 24. In: EndocrinoPEDia. 2021.
14.*** American Academy of Pediatrics. Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Pediatrics. 2016. p. 137.
15.*** La Cour D, Long D, Perlman S. Dysfunctional Uterine Bleeding in adolescent females associated with endocrine causes and medical conditions. J Pediatr Adolesc Gynecol. 2010; 23: 62-70.
16.* Khamees D, Klima J, O’Brien SH. Population screening for von Willebrand disease in adolescents with heavy menstrual bleeding, J Pediatr. 166: 195-7, 2015.
17.* Ostensen M, Almberg K, Koksvik H. Sex, reproduction, and gynecological disease in young adults with a history of juvenile chronic arthritis. J Reumatol. 2000; 27: 1783-7.
18.* Pasto SG, Mendonca BB, Bonfa E. Menstrual disturbances in patients with systemic lupus erithematosus without alkylating therapy: clinical, hormonal and therapeutic associations. Lupus. 2002; 11: 175-80.
19.* Noorhasan DJ, Weiss G. Perimenarchal menorrhagia: evaluation and Management. J Pediatr. 2010; 156: 162.
20.*** Wilkinson J, Kadir R. Management of abnormal uterine bleeding in adolescents. J Pediatr Adolesc Gynecol. 2010; 23: S22-30.
21.*** American College of Obstetricians and Gynecologists. ACOG Committee Opinion No 557: Management of acute abnormal uterine bleeding in nonpregnant reproductive-aged women. Obstet Gynecol. 2013; 121: 891-6.
22.** Haamid F, Sass AE, Dietrich JE. Heavy menstrual bleeding in adolescents, J Pediatr Adolesc Gynecol. 2017; 30: 335-40.
23.** Ryan SA. The treatment of dysmenorrhea. Pediatr Clin North Am. 2017; 64: 331-42.
24.** Youngster M, Laufer MR, Divasta AD. Endometriosis for the primary care physician. Curr Opin Pediatr. 2013; 25: 454-62.
25.** Hofmeister S, Bodden S. Premenstrual syndrome and premenstrual dysphoric disorder. Am Fam Physician. 2016; 94: 236-40.
Recommended bibliography
- Ginecología Pediátrica. Documentos de Consenso SEGO 2017 (Pediatric Gynecology. Consensus Documents SEGO 2017). Coordinator: Cancelo Hidalgo MJ. Members: Parera i Junyent N, Almansa González C, Rodríguez Jiménez MJ, Hernández de la Calle I.
Basic introduction to the physiology and gynecological pathology of children and adolescents, essential for both gynecologists and pediatricians, with the participation of the Gynecology Group for Children and Adolescents of the SEGO.
- Guía de Atención Ginecológica en la Infancia y Adolescencia. Sociedad Española de Ginecología y Obstetricia. 2013 (Gynecological Care Guide for Children and Adolescents. Spanish Society of Gynecology and Obstetrics. 2013).
Essential guide for child and adolescent gynecology consultation and adolescent pediatrics. The chapters analyzed include the pathologies that are the most frequent reason for consultation. Concise, easy to use, and with a diagnostic and therapeutic approach guide.
- Argente Oliver J, Soriano Guillén L. Manual de Endocrinología Pediátrica. 2ª ed. Madrid. Ergon. 2014. (Manual of Pediatric Endocrinology).
This manual of Pediatric Endocrinology, fundamental for the knowledge of this topic, is understandable and has an agile reading. Its diagnostic-therapeutic algorithms are of great interest for their application in daily practice.
- Pediatric Endocrinology website. Available at:
http://www.webpediatrica.com/endocrinoped/endocrinopedia.php.
Web page that is constantly updated on Pediatric Endocrinology. It is easy to navigate and contains very good diagnostic and therapeutic guidance. It is also very well documented.
- Hidalgo Vicario MI, Rodríguez Molinero L, Muñoz Calvo MT. Medicina de la adolescencia. Atención integral (3ª ed.). SEMA. Ergon. 2021. (Adolescent medicine).
Very complete work directed exclusively to adolescence. Multiple pathologies related to this stage are addressed. It includes important participation of professionals from different fields and has recently been updated.
| Clinical case |
|
Chief complaint A 16-year-old female is referred for primary amenorrhea. She refers progression of secondary sexual characteristics (breast and hair). There are no other associated symptoms. Personal history Left unilateral vesicoureteral reflux. No previous surgical interventions. No current medications. She is currently an 11th grade student. Good academic performance. Good nutrition. She does not play sports. Family background She has a healthy younger brother and healthy parents. Mother´s age of menarche was 12 years. Physical and gynecological examination Weight: 59.5 kg. Height: 169 cm. BMI: 20.83 kg/m2. Feminine fat distribution. Tanner stage IV for breasts and stage IV for axillary and pubic hair. Gynecological examination: vulva without abnormalities. No perineal alterations. Normal clitoris and urethra. Transverse hymenal septum. Mild abdominal and sacral hirsutism. Abdominal gynecological ultrasound: the uterus is not visualized by this technique. Right ovary well visualized containing follicles, it measures 38 x 18 mm. Left ovary: it is visualized with difficulty, measurements: 24 x 17 mm. Ancillary tests Blood analysis: FSH: 4.3 mIU/mL; LH: 5.8 mIU/mL; Estradiol: 177 pg/mL; Progesterone: 11.5 ng/mL. Karyotype 46 XX; MRI: complete absence of uterus and most of the vagina, except for a small outline or stump of the distal end of the vagina and vaginal vestibule with normal appearance of the labia and vulva region.
|